The registration for individual courses is now online!
Thursday, 11 June 2026

SCS Morning Run
Intuitive
Registration & Exhibition Opening
ARS - Free Communication


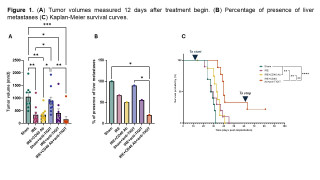
Irreversible electroporation + CD40 Agonism + TIGIT Blockade Improves Outcomes in Aggressive Orthotopic PDAC Model
Abstract
Background
Pancreatic ductal adenocarcinoma (PDAC) is an immunologically “cold” tumor with limited benefit from immune checkpoint inhibition. Irreversible electroporation (IRE) is a non-thermal local ablation therapy used in selected patients with advanced PDAC. In syngeneic orthotopic models, IRE plus intratumoral (IT) CD40 agonist antibody (CD40 Ab) showed anti-tumor immune effects and reduced liver metastases; this regimen is currently under clinical evaluation. TIGIT is an immune checkpoint that is highly co-expressed with PD-1 on infiltrating T cells in PDAC after IRE.
Aims
To evaluate whether systemic adjuvant TIGIT blockade (anti-TIGIT) improves outcomes after IRE+CD40 Ab in an aggressive orthotopic PDAC model.
Methods
Spontaneously metastasizing KPC46 PDAC organoids were implanted into the pancreatic tail of mice via laparotomy. When tumors reached approximately 7 mm, mice were randomized to sham laparotomy, IRE, IRE+CD40 Ab, sham+anti-TIGIT, IRE+anti-TIGIT, or IRE+CD40 Ab+anti-TIGIT (n=8-10/group). Immediately after IRE, CD40 Ab (50 µg) was administered IT once. Anti-TIGIT Ab (100 µg) was administered intraperitoneally every other day starting 48 hours post-IRE. Mice were euthanized on day 12 for assessment of tumor burden and immune profiling by flow cytometry. Survival cohorts included sham laparotomy, IRE, IRE+CD40 Ab, and IRE+CD40 Ab+anti-TIGIT.
Results
All IRE-treated groups showed smaller primary tumor volumes versus sham, with the greatest reduction after IRE+CD40 Ab+anti-TIGIT (Figure 1A). Flow cytometry demonstrated the largest reduction in regulatory T cells and the greatest increase in natural killer cells with triple therapy (not shown). These immune changes were associated with reduction in liver metastases on day 12 (Figure 1B). IRE+CD40 Ab+anti-TIGIT also improved survival over other groups with 22% complete responders (Figure 1C).
Conclusion
Adding systemic anti-TIGIT Ab to IRE+CD40 Ab improves local control, remodels the tumor immune microenvironment, reduces liver metastases, and prolongs survival. Ongoing experiments include rechallenging tumor-free surviving mice and comparison of anti-TIGIT to other immune checkpoint strategies.
Automating the Comprehensive Complication Index with Artificial Intelligence: Evaluation of Quality and Clinical Potential
Abstract
Background
The Comprehensive Complication Index (CCI) is a validated, clinically established, and sensitive measure of postoperative morbidity but is underutilised due to the labor-intensive and error-prone nature of manual complication extraction and grading. Large language models (LLMs) can analyse free-text surgical discharge summaries and accurately apply the Clavien-Dindo Classification (CDC). However, their ability to reliably compute the more complex CCI – requiring identification of multiple events, correct severity grading and weighted aggregation – remains unclear.
Aims
To evaluate the feasibility and accuracy of contemporary LLMs in extracting postoperative complications and computing the CCI from unstructured surgical discharge summaries.
Methods
Six LLMs (ChatGPT-5.2, Claude Sonnet 4.5, DeepSeek-V3.2, Mistral AI (2024), Gemini 3 Flash and Llama 4) were assessed using a tiered validation framework. After conceptual testing, each model analysed 20 de-identified real-world surgical discharge summaries. A three-layered prompting framework (preprocessing, complication extraction and computation, and consistency checking) was compared with naïve end-to-end analysis. Agreement with expert reference CCI values was assessed using intraclass correlation coefficients (ICC) and Bland-Altman analysis.
Results
All models correctly defined the CCI concept. Naïve analysis showed moderate agreement with reference CCI values (ICC(3,2) = 0.87), with the observed disagreement being driven by missed complications and incorrect aggregation. Structured prompting improved agreement to excellent (ICC(3,1)=0.93) with minimal systematic bias. ChatGPT and Claude achieved full agreement with reference CCI values across all cases. Discrepancies in other LLMs were attributable to ambiguity in clinical documentation or inherent interpretive boundaries of the CCI framework, rather than computational errors.
Conclusion
LLMs can accurately extract complications, assign CDC grades, and compute CCI from unstructured free-text surgical discharge summaries when guided by structured prompting. This demonstrates that AI can reliably perform complex morbidity aggregation and may reduce clinical workload while improving standardization of surgical outcome reporting. Further large-scale validation is warranted.
Two Actionable Windows: Disentangling Early Mortality from Late Infection Risks Using Time-Resolved AI
Abstract
Background
Postoperative mortality and infection are frequently monitored using uniform clinical and laboratory strategies, despite likely arising from distinct pathophysiological mechanisms. Current one-size-fits-all monitoring may obscure actionable signals and limit the effectiveness of preventive interventions.
Aims
To disentangle the temporal and physiological drivers of early postoperative mortality and late postoperative infection using time-resolved, explainable machine-learning models, and to identify distinct postoperative risk windows to inform phase-specific clinical interventions.
Methods
We trained outcome-specific machine-learning models for 30-day mortality and postoperative infection using a retrospective cohort of 32,328 surgical episodes across seven specialties. Models integrated baseline patient characteristics with daily laboratory trajectories from postoperative days (POD) 0–7. Explainable AI techniques were used to quantify time-dependent feature importance, enabling differentiation between early “state”-driven risks and later “trajectory”-driven risks.
Results
Event rates were 4.6% (1,471/32,328) for mortality and 16.6% (5,374/32,328) for infection. Two distinct postoperative risk phases were identified.
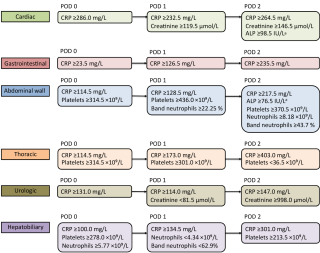
Rescue window (POD 0–2): Mortality risk was front-loaded, driven by baseline vulnerability and acute physiological derangements, particularly changes in haemoglobin (bleeding and transfusion) and creatinine (renal dysfunction), with maximal influence within the first 48 hours.
Surveillance window (POD 3–7): Infection risk emerged later and was driven by evolving inflammatory trajectories rather than baseline state. Key predictors included CRP kinetics, platelet rebound patterns, and persistent dysglycaemia.
Conclusion
Postoperative mortality and infection exhibit distinct temporal and physiological signatures. A phase-specific care model is warranted, prioritizing hemodynamic stabilization and renal protection during the early rescue window (POD 0–2), followed by focused surveillance of inflammatory trajectories during the surveillance window (POD ≥3) to enable early infection detection. This framework supports a transition from generic postoperative monitoring to precision, time-adapted care.
End-of-Surgery Prediction of Postoperative Infectious Complications Using Intraoperative Vital-Sign Dynamics
Abstract
Background
Postoperative infections remain a leading cause of morbidity, yet risk stratification is often delayed until postoperative laboratory data becomes available. This leaves a critical decision window immediately after surgery unsupported by objective risk assessment.
Aims
To evaluate whether intraoperative physiological instability, captured through high-frequency vital-sign data, can predict postoperative infectious complications immediately at the end of surgery.
Methods
We developed a machine-learning framework using a retrospective cohort of 15,330 surgical procedures. The model integrated standard preoperative factors with intraoperative time-series data (heart rate, blood pressure, SpO₂, EtCO₂, and temperature). Beyond simple averages, we engineered interpretable dynamic features including trend stability, entropy, skewness, and kurtosis to capture higher-order physiological complexity. Model performance was evaluated using AUROC and calibrated across procedure clusters, with SHAP analysis used to identify key predictive drivers.
Results
Postoperative bacterial infection occurred in 515 (4.7%) procedures. While a model based solely on preoperative factors achieved an AUROC of 0.75, the inclusion of intraoperative vital-sign dynamics significantly improved discrimination to an AUROC of 0.86 (95% CI 0.85–0.89). Crucially, this end-of-surgery model approached the accuracy of models incorporating POD 2 laboratory data (AUROC 0.89) but provided risk stratification 48 hours earlier. Key physiological drivers included blood pressure instability (high kurtosis), baseline temperature deviations, and the cumulative burden of hypoxia.
Conclusion
Intraoperative vital-sign dynamics serve as a powerful digital biomarker, enabling the prediction of infectious complications immediately at skin closure. This approach allows for targeted triage such as enhanced monitoring or early bundle activation in the recovery room, days before clinical symptoms or laboratory abnormalities appear.
AI-Guided Postoperative Infection Surveillance: Lab Test Recommendations by Postoperative Day
Abstract
Background
Early detection of postoperative bacterial infections is critical for improving surgical outcomes, yet current laboratory testing strategies are largely empirical and not procedure-specific. Leveraging large-scale electronic health record (EHR) data may enable evidence-based recommendations for optimized laboratory monitoring.
Aims
To derive and validate procedure-specific, data-driven recommendations for the selection, timing, and diagnostic thresholds of laboratory tests for early detection of postoperative bacterial infections.
Methods
This retrospective cohort study was conducted at an academic hospital and included surgical cases performed between May 2014 and September 2022. A consecutive sample of 91794 surgical procedures across 12 specialties was extracted from the EHR. Exclusion criteria were infection present on admission, missing diagnostic codes or unassignable to a procedure category, resulting in 32328 surgeries included in the final cohort. Each surgery was treated as an independent clinical episode.
Parameters from the preoperative (age, sex, American Society of Anesthesiologists (ASA) score, comorbidities) and intraoperative (surgery duration, emergency status, ICU transfer, antibiotic administration) phases were used to define baseline characteristics. A total of 6 postoperative laboratory markers were selected in the predictive models according to imputation performance. The primary outcome was the occurrence of any postoperative bacterial infection. The predictive model was designed to determine which laboratory tests, including their optimal thresholds, should be performed on which specific postoperative day (POD), tailored to defined surgical procedure groups.
Results
The model achieved an AUROC of 0.79 on PODs 0-2 in the pooled cohort and recommended C-reactive protein for measurement across all procedure groups. Procedure-specific relevant markers included alkaline phosphatase, creatinine, platelets, and neutrophils. Clinicians’ infection suspicion and testing practices can be observed from the use of C-reactive protein and neutrophils.
Conclusion
AI-guided analysis of routine EHR data, enables surgery-specific postoperative laboratory testing strategies. This approach allows to improve prediction of postoperative infection while optimizing resource utilization.
Getting to the Root of the Problem: Surgical RCTs Are Poorly Designed Preventing Conclusive Decision Making
Abstract
Background
Surgical randomized controlled trials (RCTs), although considered the gold standard for generating causal evidence, are often reported incompletely and inconsistently. We hypothesize that poor reporting may reflect a more fundamental problem, namely inadequate trial planning for informing clinical practice.
Aims
To examine the extent to which clinical relevance is considered in the aim and design, definition of primary and secondary endpoints, and interpretation in surgical RCTs.
Methods
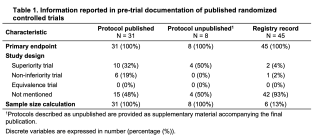
We conducted a systematic literature search to identify all RCTs using the Comprehensive Complication Index® as an endpoint. From pre-trial documentation and final publications, we extracted information on study aims, design, endpoints, and sample size calculations. For trials with a statistically significant primary endpoints, we assessed whether results were interpreted in terms of clinical relevance.
Results
We identified 87 published RCTs. Pre-trial documents were available for 84(98%) trials; all defined a primary endpoint, but only 23(27%) reported the study design. Among the final publications, 20(23%) trials specified an aim to show superiority with a corresponding study design and 12(14%) a non-inferiority aim and design. The remaining 55 trials did not report a study aim but were basically designed and conducted as superiority trials. Sample size calculations were provided in 84(98%) trials, and 44(51%) achieved statistical significance for their primary endpoint. Of these, only 9(20%) interpreted their results from a clinical perspective.
Conclusion
Although endpoints and sample size calculations were usually reported, specific study aims and corresponding design as well as clinical interpretation were frequently lacking. More than half of trials failed to demonstrate superiority and might have offered more meaningful guidance to clinical practice if designed as non-inferiority trials. These findings highlight limited awareness of study planning that clearly specifies appropriate aims-such as superiority or non-inferiority for different outcomes-to adequately assess the balance between beneficial and harmful effects when comparing surgical interventions.
Quantification of Islet Cell Cluster Size Heterogeneity in the Juvenile Porcine Pancreas
Abstract
Background
While whole-organ pancreas and islet allotransplantations offer effective alternatives for type 1 diabetes (T1D) treatment, their clinical use is limited by the shortage of human donors. Xenotransplantation is a potential solution to this challenge, with porcine pancreases emerging as an up-and-coming alternative source of islets. While neonatal or juvenile piglets are becoming increasingly favored for obtaining pancreatic islets, no optimal age for clinical application has been established. Debates continue regarding the islet size and function, which are mostly considered immature and are thus referred to as islet cell clusters (ICCs).
Aims
This study investigated the ICC size heterogeneity in tissue samples from six juvenile porcine pancreases, all 14 days of age.
Methods
The abundance of ICCs of different sizes (defined as small, intermediate, and large) was assessed in large images of pancreas sections. Automated workflows using NIS Elements software were developed to measure and cluster areas of immunofluorescent-stained beta- and alpha-cells, and to quantify the proportions of insulin- and glucagon-positive regions within the different-sized clusters.
Results
Small, well-developed islets (~100 μm) were consistently identified across all juvenile pancreases, with a density of 6.2 ± 2.5 clusters/mm² (Mean ± S.D.). Homogeneous numbers of intermediate-sized (14.3 ± 4.6 clusters/mm²) and small-sized (72.2 ± 12.6 clusters/mm²) clusters were also observed. Insulin staining predominated in small and intermediate clusters (4-fold higher than glucagon), while large clusters exhibited significantly more glucagon staining, consistent with characteristics of mature islets.
Conclusion
Although further studies are needed to confirm the clinical suitability of juvenile porcine ICCs, our findings suggest that 14-day-old piglets already possess significant amounts of small, mature islets. Optimizing islet isolation techniques, such as gradient centrifugation used in human islet isolation, may enable efficient purification of small islets from juvenile porcine pancreases for transplantation.
Systemic Translocation of Small Intestinal Microbiota as a Source of Surgical Site Infections
Abstract
Background
Surgical site infections (SSIs) after abdominal surgery remain a leading cause of postoperative morbidity and mortality despite meticulous preoperative skin disinfection. The bacterial origin of SSIs and routes of dissemination remain unclear.
Aims
To determine the potential intestinal origin and dissemination routes of bacteria causing SSIs after abdominal surgery and to identify microbiota-associated intestinal risk signatures and modifiable preoperative nutritional factors that predispose patients to SSIs.
Methods
We performed metagenomic sequencing of small intestinal specimens and strain-resolved sequencing of matched bacterial isolates from the small intestine, mesenteric lymph nodes (MLNs), and infected surgical sites in patients undergoing pancreatic resection. Deep preoperative nutritional phenotyping was conducted to identify dietary patterns associated with intestinal microbiota states and SSI risk.
Results
This cross-compartment approach revealed clonal continuity of bacterial isolates from the small intestine through the MLNs to the postoperative infection site, demonstrating MLN-mediated bacterial translocation as a direct dissemination route. Metagenomic profiling of small intestinal contents at surgery further showed that reduced microbial diversity and Enterococcus dominance strongly predicted SSI risk. Preoperative dietary analysis identified high-fat intake as a key modifiable factor associated with this dysbiotic, infection-prone small intestinal state.
Conclusion
Together, our findings show an endogenous origin of SSIs in the small intestine and indicate translocation through MLNs as the route of infection. This endogenous source of SSIs opens the field for novel measures to prevent SSIs, including identification of patients at risk, dietary interventions and tailored antimicrobial prophylaxis.
Blunt & Penetration Thoracic and Abdominal Trauma


Advances in Managing Thoracic Trauma: Role of VATS in Chest Trauma
Role of Laparoscopy in Abdominal Trauma
Modern Rib Fracture Management
What Can We Learn From Australia’s Approach
From Cutting to Connecting: Sharing, Learning, Progressing
HPB I

Circulating tumor DNA and neoadjuvant therapy in localized Pancreatic Ductal Adenocarcinoma – A systematic review and meta-analysis
Abstract
Background
ctDNA is increasingly investigated as a biomarker in pancreatic ductal adenocarcinoma (PDAC), but its role in guiding treatment decisions before, during, and after neoadjuvant treatment (NAT) remains unclear.
Aims
This study aims to synthesize the current evidence on the predictive value of ctDNA in localized pancreatic ductal adenocarcinoma PDAC, with a particular focus on its potential to guide clinical decision-making before, during, and after NAT.
Methods
A systematic review and meta-analysis (Prospero: CRD420251013013) of studies evaluating ctDNA in patients with localized PDAC treated with NAT was conducted. Meta-analyses were performed for OS and PFS when ≥2 studies reported outcomes.
Results
15 studies, representing 926 patients, met the inclusion criteria. Five studies measured ctDNA using a PCR-only assay, five using only NGS, and four studies used both methods. All studies targeted KRAS mutations for ctDNA assessment, with substantial heterogeneity in assay platforms, thresholds, and sampling timing. Baseline ctDNA detection ranged from 11-73% across resectability categories. Baseline ctDNA positivity was associated with worse PFS (2 studies, pooled HR 2.34, 95% CI 1.21-4.54), but association with OS could not be demonstrated (3 studies, pooled HR 1.50, 95% CI 0.96-2.37). An association between post-NAT ctDNA status and PFS or OS could not be quantitatively investigated. Postoperative ctDNA positivity was associated with inferior OS (2 studies, pooled HR 6.39, 95% CI 1.94-21.01).
Conclusion
Evidence supporting ctDNA as a biomarker to guide NAT in localized PDAC is limited and inconsistent. Postoperative ctDNA was strongly associated with poor OS, whereas larger studies are needed to assess baseline and post-NAT ctDNA.
The Validation of a Non-Invasive Genetic Biomarker Signature of Prospective Survival in Patients After Pancreatic Cancer Resection
Abstract
Background
Pancreatic ductal adenocarcinoma (PDA) is associated with poor prognosis despite surgical resection. Reliable, non-invasive biomarkers to predict tumour biology and postoperative survival are lacking. Germline single nucleotide polymorphisms (SNPs) in the CD44 and CHI3L2 genes have previously been proposed as predictive biomarkers but require independent validation.
Aims
Validation of prognostic value of CD44 rs353630 and CHI3L2 rs684559 SNPs for tumour-related survival after pancreatic resection in an independent cohort.
Methods
This retrospective validation study used prospectively collected clinical and genomic data from the International Cancer Genome Consortium Accelerating Research in Genomic Oncology (ARGO) Pancreatic Cancer–Canada cohort. Patients with resected PDA, complete survival and genotype data were included. Survival analyses were performed using Kaplan–Meier estimates and Cox proportional hazards models adjusted for American Joint Committee on Cancer (AJCC) stage.
Results
A total of 235 patients were analysed. Carriers of the major G allele at CHI3L2 rs684559 had a significantly lower risk of tumour-related death compared to A/A homozygotes (hazard ratio [HR] 0.44, 95% confidence interval [CI] 0.25–0.78; p = 0.005). For CD44 rs353630, heterozygous carriers showed a reduced mortality risk compared to A/A homozygotes (HR 0.41, 95% CI 0.17–0.98; p = 0.044). A combined risk model demonstrated that patients carrying risk-indicating genotypes of either SNP had more than a twofold increased risk of tumour-related death (HR 2.21, 95% CI 1.38–3.55; p = 0.001).
Conclusion
This study independently validates a germline SNP-based biomarker signature as a predictor of survival after pancreatic cancer resection. These findings support the clinical potential of non-invasive genetic markers for patient stratification and personalised surgical decision-making.
Impact of Vascular Encasement on Survival Outcomes in Patients with Arterial Contact ≥ 90°
Abstract
Background
Pancreatic cancer is primarily staged by the extent of tumor vessel involvement. Despite the central role of resectability classifications in clinical decision-making, these criteria have not been conclusively validated, and variation exists across classification systems.
Aims
This study investigated whether increasing degrees of baseline arterial tumor contact are associated with overall survival (OS) among patients with ≥ 90° arterial vessel contact.
Methods
Patients in the Netherlands between 2012 and 2017 classified as locally advanced pancreatic cancer according to the Dutch Pancreatic Cancer Group (DPCG) criteria with ≥90° arterial contact were included after central radiologic review of baseline CT scans. Patients were stratified by arterial encasement (90-180°, 180°-270°, and 270-360°). OS was analyzed using uni- and multivariable Cox proportional hazard models, adjusting for venous involvement and clinical covariates.
Results
Among 481 patients, 153 (31.8%) had 90-180°, 51 (10.6%) had 180-270°, and 277 (57.6%) had 270-360° arterial encasement. Resection was performed in 33 patients (6.9%): 16 (10.5%) for 90-180°, 4 (25.5%) for 180-270°, and 13 (4.7%) for >270° arterial contact. The median OS was 9.63 months for all patients and similar across groups: 9.43, 8.97, and 10.45 months (p=0.34). In univariable analysis, the extent of arterial contact was not associated with worse OS (180–270° vs. 90–180°: HR 1.25, 95% CI 0.91–1.73; 270–360° vs. 90–180°: HR 1.02, 95% CI 0.83–1.24). Increasing venous involvement rather than arterial involvement was an independent poor prognostic factor for OS (180–270° vs. <90°: HR 1.72, 95% CI 1.03–2.87).
Conclusion
Among patients with pancreatic cancer and ≥90° arterial tumor contact, increasing degrees of arterial encasement were not associated with worse OS. These findings suggest that, beyond 90 degrees of arterial involvement, anatomical extent alone poorly reflects prognosis and support integrating biological and patient-specific factors to guide treatment decisions for LAPC.
Perioperative real time glucose assessment as a predictive tool for complications after pancreatic resection in non-diabetic patients- A prospective single center pilot study
Abstract
Background
Postoperative hyperglycaemia has been described as an early marker of complications after pancreatic resection. However, evidence is based on retrospective assessment of arbitrary serum glucose measurements. In contrast, continuous glucose monitoring (CGM) systems allow real-time monitoring of glucose fluctuations.
Aims
The aim of this study is to investigate continuous perioperative glucose changes after pancreatic resection and the impact on postoperative complications.
Methods
Twenty (n=20) consecutive patients undergoing pancreatic resection were prospectively enrolled. In addition, n=10 patients undergoing other major abdominal surgery served as control group. Dexcom G6 CGM system was used. Time in euglycemic range (TIR) and peak glucose levels were analyzed. Routine serum glucose measurements and daily C-reactive protein (CRP) levels were also assessed. Comprehensive Complication Index (CCI) was used to quantify postoperative complications.
Results
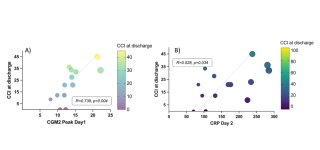
No adverse events related to CGM devices were observed. Glucose levels increased significantly from a median of 7mmol/l (IQR 6-8mmol/l) to 9 mmol/l (IQR 8-1mmol/l, P=0.026) after pancreatic resection. Correspondingly, the TIR decreased from 86.5% (IQR 85-96%) to 78.1% (IQR 34-89%, p=0.042). Perioperative glucose levels (p=0.623) and TIR (p=0.408) remained unchanged in the control group. Linear regression showed a significant correlation between peak glucose levels on day 1, measured by CGM (R=0.738, p=0.004, Figure 1A), and CRP levels on day 2 (R=0.528, p=0.034, Figure 1B) with CCI. In contrast, routine serum glucose levels did not predict complications.
Conclusion
In this pilot study, peak glucose levels on day 1 after pancreatic resection were associated with adverse events. CGM may be a valuable tool to identify patients at risk of complications.
Hepatico-jejunostomy during pancreatic surgery is a safe teaching procedure for young trainees: a multivariable analysis
Abstract
Background
The reconstructive phase of pancreatic surgery may be suitable for teaching young general surgery trainees in performing hepatico-jejunostomy (HJ).
Aims
Describe the technique, and the results of HJ in a teaching hospital.
Methods
Retrospective analysis of consecutive pancreatoduodenectomy (PD) and total pancreatectomy (TP) from 01/2016 to 10/2025. The primary outcome was a composite-endpoint of HJ-related morbidity (primary biliary leak, cholangitis/sepsis or abscess, HJ stenosis) in HJ performed by seniors vs. trainees. Cox regression analysis was used to assess the predictors of HJ-related complications including teaching among covariates.
Results
During 150 pancreatic resections (PD=145; TP=5), 115 HJ (76.7%) were taught to a total of 22 trainees of postgraduate year≥4 (mean HJ number=5.2 per trainee).
Patient baseline and bile ducts characteristics were similar for seniors vs. trainees. A single-layer HJ with 5-0 or 6-0 absorbable monofilament was performed in all cases, using interrupted sutures in 86%.
After a median follow-up of 20.3 months (IQR 8.4-39.5), HJ-related morbidity rate was 10.0% (cholangitis 8.7%, biliary leak, abscess and stenosis 0.67% each). HJ-related morbidity was 11.4% vs. 9.6% for the seniors vs. the trainees respectively (p=0.751), without differences in biliary leaks, cholangitis, abscesses, nor stenosis (all p>0.05).
Percutaneous biliary drainage was needed in 2 cases (1.3%), and surgical reintervention in 2 (1.3%). For redo-surgery, 1 was due to primary biliary leak successfully managed using a trans-anastomotic T-tube, the other was conversion of HJ to a Roux-en-Y loop due to persistent biliary reflux and recurrent cholangitis 1-year after PD. In both cases HJ was performed by a senior surgeon. Overall, HJ-related reinterventions were similar for seniors vs. trainees (5.7% vs 1.7%; p=0.232). Redo-HJ was never necessary. Cox regression analysis showed that the cumulative-risk of HJ-related morbidity was not impacted by teaching.
Conclusion
Respecting the technical principles of HJ ensures the feasibility and safety of teaching bilioenteric reconstruction during pancreatic surgery.
Update on post-recurrence survival after pancreatic cancer resection: a comprehensive systematic review
Abstract
Background
The burden of recurrence after resection of pancreatic-ductal-adenocarcinoma (PDAC) remains very high, leading to a dismal prognosis. Post-recurrence survival (PRS) and its determinants have been less studied compared to traditional outcomes like overall and recurrence-free survival.
Aims
To provide an update on PRS after PDAC resection and identify its prognostic determinants.
Methods
A PRISMA-compliant systematic literature review was performed, searching studies published in the period January 01/2010-12/2025 (PubMed/Scopus/Web of Science). The population, intervention, comparator, outcome (PICO) strategy was used to formulate study questions and select studies: Population/Intervention) original studies including patients who had resection of non-metastatic PDAC and specifically reporting PRS; Comparator) timing/pattern/treatment of recurrence; Outcomes) PRS defined as survival after PDAC recurrence, site- and treatment-specific PRS, predictors of PRS.
Results
Forty-five eligible studies were identified. Median PRS range was 2.6-44.0 months. Local recurrence (remnant pancreas or locoregional lymph nodes) and lung-limited recurrence had longer PRS (range, 5.0-20.0 months and 8.5-32.5 months respectively) compared to liver recurrence (range, 5.1-8.5 months). Peritoneal or multisite recurrence had the shortest PRS. Whenever oncologically/technically feasible, completion pancreatectomy (i.e., isolated local recurrence), and resection of limited recurrence in the lungs or regional/retroperitoneal lymph nodes were associated with longer PRS, compared to systemic treatment alone. Combined local and systemic treatment had a positive effect on PRS, compared to systemic chemotherapy alone.
Prolonged PRS was associated with asymptomatic recurrence or low performance status, routine/active follow-up, longer recurrence-free survival after first pancreatectomy, lung-only/isolated local recurrence, resectable recurrence, young age, serum albumin and Ca19-9 levels at recurrence, adjuvant chemotherapy after index pancreatectomy.
Conclusion
PRS varies widely based on pattern/timing/treatment of recurrences. Systemic control of the disease is pivotal. Patients eligible for radical treatments (i.e., completion pancreatectomy) or showing favorable tumor biology (isolated lung recurrence), may achieve very long PRS. The impact of neoadjuvant therapy (before index pancreatectomy) on PRS is still unexplored.
In-depth analysis of post-recurrence survival in resected pancreatic ductal adenocarcinoma: a cohort study
Abstract
Background
Recurrence after curative-intent resection of pancreatic ductal adenocarcinoma (PDAC) is frequent, however post-recurrence survival (PRS) may vary widely.
Aims
To analyze in depth PRS and identify the prognostic factors associated with it.
Methods
Retrospective cohort study including patients with PDAC recurrence after pancreatectomy. PRS was estimated with the Kaplan Meier method in the whole cohort and in subgroups based on performance status (ECOG-PS) at recurrence, timing, pattern, treatment of recurrence. Prognostic factors of PRS were evaluated through a Cox regression model.
Results
Seventy patients who underwent pancreatic resection (pancreatoduodenectomy, n=49; distal pancreatectomy, n=19; total pancreatectomy, n=2), and experienced PDAC recurrence, were included. R0, pN+ and perineural invasion rates were 72.9%, 67.1% and 94.3% respectively. Neoadjuvant and adjuvant chemotherapy were administered in 34.3% and 70% respectively. Recurrences were in multiple sites (51.4%), peritoneal-only (18.6%), hepatic-only (7.1%), isolated local (11.4%), pulmonary-only (1.4%). Early recurrence (<1 year after pancreatectomy) occurred in 41 cases (58.6%). Mean recurrence-free survival was 14.0 months; mean PRS was 13.0 months in the whole cohort.
In subgroup analyses, patients with low ECOG-PS (0-1) had longer PRS than those with high ECOG-PS (>1) (log-rank=42.1; p>0.001). Conversely, PRS was similar in patients in early vs. late recurrences (log-rank=1.110; p=0.292) and by site of recurrence (log-rank=2.39; p=0.664). Recurrence treatment with chemotherapy, radical surgery or both was associated with longer PRS compared to radiotherapy, palliative surgery or best supportive care (log-rank=35.7; p<0.001). Cox regression analysis found R0 resection after index pancreatectomy (HR=0.44), low ECOG-PS at recurrence (HR=0.18) and treatment of recurrence by chemotherapy, surgery or both (HR=0.34), to be independently associated with a lower cumulative risk of death after recurrence. Borderline/locally-advanced PDAC and multisite recurrences tended toward worse PRS.
Conclusion
PRS seems influenced by patients' conditions at recurrence and the feasibility of effective treatments (including surgery), rather than only by surrogates of biology of the disease (initial resectability status, timing/pattern of recurrence).
Benefit of Adjuvant Chemotherapy for Resected Pancreatic Cancer Following Neoadjuvant FOLFIRINOX or Gemcitabine-Nab-Paclitaxel: A Multinational Analysis
Abstract
Background
Neoadjuvant therapy (NAT) has become the standard of care for borderline resectable (BRPC) and locally advanced pancreatic cancer (LAPC). However, the survival benefit of adjuvant therapy (AT) following curative resection in this setting remains controversial, particularly regarding the optimal regimen selection.
Aims
To investigate the association between AT and overall survival (OS) in patients with resected BRPC and LAPC, specifically stratified by the type of NAT regimen received (FOLFIRINOX vs. Gemcitabine/Nab-paclitaxel).
Methods
This multinational, 19-center retrospective cohort study included patients with resected BRPC or LAPC who completed NAT with either FOLFIRINOX or Gemcitabine/Nab-paclitaxel (Gem/Nab). Propensity score matching (PSM) was utilized to minimize selection bias between patients receiving AT versus observation. The primary outcome was OS.
Results
The study included 834 patients (605 NAT FOLFIRINOX; 229 NAT Gem/Nab). In the NAT FOLFIRINOX cohort, the administration of adjuvant FOLFIRINOX was associated with significantly longer OS in the matched analysis (Median OS: 42.0 vs 25.8 months; Hazard Ratio [HR]: 0.58; 95% CI, 0.43-0.79; p<0.001). Notably, this survival benefit was observed regardless of nodal status, extending to node-negative (pN0) patients. Conversely, switching to adjuvant Gem/Nab after neoadjuvant FOLFIRINOX provided no survival benefit (HR 0.84; p=0.27). In the NAT Gem/Nab cohort, the addition of adjuvant chemotherapy (either Gem/Nab or other regimens) was not associated with improved OS (HR 0.92; p=0.69).
Conclusion
The survival benefit of adjuvant chemotherapy in resected BRPC and LAPC appears to be regimen-dependent. Continuation of FOLFIRINOX in the adjuvant setting is associated with improved survival for patients successfully inducted with FOLFIRINOX, independent of pathological nodal status. However, de-escalation to gemcitabine-based regimens after neoadjuvant FOLFIRINOX or administering adjuvant therapy following NAT Gem/Nab does not appear to confer a significant survival advantage.
Joining Forces – Colorectal Emergencies
The Many Ways to Manage Perforated Diverticulitis
What to Do in Left-Sided Colonic Obstruction
How to Join Forces in Lower Gastrointestinal Bleeding
We Have a Proctologic Emergency
When and How to Operate in Bowel Occlusion in Peritoneal Carcinomatosis
Joining Forces – Treatment of Colorectal Liver Metastases – What's the Best Approach/Treatment?

When Which Surgical Resection?
Is Transplantation an Option?
Where Ablation Beats Surgery?
Case Discussions
Joining Forces within Pediatric Surgery: From Head to Toe

Postoperative Outcomes of Endoscopic Third Ventriculostomy in Pediatric Patients
Abstract
Background
Endoscopic third ventriculostomy is an established surgical treatment for pediatric hydrocephalus, particularly in obstructive cases. However, reported success rates vary widely, and the influence of patient age at the time of surgery remains controversial.
Aims
This study aimed to evaluate postoperative outcomes of endoscopic third ventriculostomy in children, with a particular focus on treatment failure over time and the impact of age at surgery.
Methods
A retrospective cohort study was conducted including all pediatric patients who underwent endoscopic third ventriculostomy between January 2017 and October 2023 at a single tertiary pediatric center. Demographic data, perinatal characteristics, operative details, and postoperative outcomes were collected from electronic medical records and analyzed pseudonymously. Endoscopic third ventriculostomy was considered successful if patency was maintained during follow-up or restored by revision; irreversible failure or subsequent shunt placement was defined as treatment failure. Survival analysis was performed using Kaplan–Meier curves, and groups were compared using log-rank testing.
Results
Twenty-eight patients were included, of whom 64.3% were male. Median age at surgery was 4.5 months, with 71.4% of patients operated on before one year of age. During follow-up, 17.9% of endoscopic third ventriculostomies remained patent. Primary treatment failure occurred in 25.0% of patients, while secondary failure was observed in 57.1%. Median time to failure of 50% of procedures was 91 days, and after 360 days, 25.0% of patients remained shunt-free. Patients operated on after the first year of life showed a tendency toward improved endoscopic third ventriculostomy survival compared with younger patients; however, this difference did not reach statistical significance (hazard ratio 0.88, p = 0.80).
Conclusion
Endoscopic third ventriculostomy represents an important treatment option for pediatric hydrocephalus but is associated with considerable failure rates during long-term follow-up. Patient age at surgery appears to influence postoperative outcomes, with a trend toward better results in older children. Careful patient selection is essential, and further prospective studies are needed to refine indications and optimize outcomes.
Optimizing Fracture Care in Children Using Biodegradable Magnesium Screws: Healing and Complications During Fixation With Magnesium Screws – A Retrospective Pilot Study
Abstract
Background
Fractures in childhood are quite common. Approximately 15-45% of children experience a fracture during their growth phase. Fortunately, only a few require osteosynthesis. This typically represents a stressful situation for the family, as surgery and especially removal of osteosynthesis material is associated with complications and high costs. Therefore, resorbable osteosynthesis materials are gaining increasing attention. Due to their beneficial material properties, magnesium screws (ZX00) are increasingly used in the pediatric population.
Aims
The aim of this study was to evaluate fracture healing and complications in fractures treated with magnesium screws and to compare them with those treated using conventional screws.
Methods
Retrospective analysis of fractures treated with magnesium screws versus conventional osteosynthesis in a 1:2 matched-pairs design. For this purpose, the RemeOs screw (Bioretec) was used to treat epi-metaphyseal fractures of the long bones as well as fractures of one or more bones of the hand or foot. Radiological consolidation, range of motion (ROM), and complications were evaluated over the same follow-up period as patients treated with conventional screws.
Results
To date, seven patients have been treated with magnesium screws. All patients show timely consolidation and symmetrical mobility compared to the control group. No complications have occurred so far. At present, the available data are insufficient for a representative analysis. However, the preliminary results are encouraging.
Conclusion
This pilot study shows that magnesium screws could optimize pediatric fracture treatment. Initial results are promising, as radiological and clinical fracture consolidation was observed in all patients. Therefore, hardware removal is no longer necessary. However, the effects of these screws on cartilage and the growing skeleton in different fracture types (e.g. radial condyle fractures) require careful evaluation in long-term follow-up studies.
Extended Minimal Invasive Craniectomy in Sagittal Synostosis – Is it Worth it?
Abstract
Background
Since 2017, we have been performing endoscopy assisted craniectomy for craniosynostosis, with approximately half of the 100 treated patients presenting with sagittal synostosis. Initially, only a narrow bone strip between the coronal and lambdoid sutures was removed. In 2022, we modified our approach by extending the craniectomy into the occiput, similar to our open technique.
Aims
The aim of this study was to evaluate the effect of this modification on perioperative and postoperative outcomes.
Methods
We analyzed all patients who underwent endoscopy assisted surgery for sagittal synostosis between 2017 and 2024, dividing them in two groups, according to surgical technique. We compared age and skull index at surgery, duration of surgery and hospital stay, blood loss and transfusion rate, as well as skull index at the and of the helmet therapy and one year later and duration of helmet therapy.
Results
Between 2017 and 2024, 50 children with sagittal synostosis underwent endoscopy assisted craniectomy. 45 had complete data for analysis. By mid-2022, 25 children underwent the previous technique, since then 20 patients the extended procedure. Age and initial skull index in the two groups did not differ significantly. At the end of the helmet therapy, the skull index was 2 points higher in the extended technique group and even 3 points higher 1 year later. The extension of the craniectomy increased the duration of surgery by 10 minutes, while there was no adverse effect on the duration of hospitalization, blood loss or need for transfusion.
Conclusion
Expanding the craniectomy improves the outcome after minimal invasive craniectomy in sagittal synostosis and should be considered at least in more severe cases, although a slightly longer duration of surgery has to be accepted.
A Low-Cost Rubber Plunger Simulator for Pediatric Minimally Invasive Surgery
Abstract
Background
In neonatal minimally invasive surgery (MIS), as well as in pediatric retroperitoneoscopic procedures, the working volume is highly restricted.
Aims
The objective was to design and validate a new, low-cost, and reproducible dry lab model that realistically reproduces not only the limited workspace but also the characteristics of the abdominal wall including the curvature of its surface and its mechanical behaviour for neonatal MIS skills training.
Methods
The model consists of a rubber plunger with a base diameter of 11 cm and an internal height of 6 cm, corresponding to an internal volume of slightly less than 500 ml. Selected laparoscopic exercises were performed inside the plunger using 3 mm short pediatric instruments (Karl Storz) and a 5 mm 30° laparoscope. Validation of the model was performed during a national pediatric surgery congress course in June 2025. Data were collected from participants using a 5-point Likert scale questionnaire based on the Michigan Standard Simulation Experience Scale (MiSSES) and subsequently analyzed.
Results
Twelve course participants were recruited (9 females: 3 males). Seven (58%) had experience with <20 MIS cases, while 5 (42%) had more extensive experience. The mean perceived degree of realism was 4.17 ± 0.58 and for environment 4.58 ± 0.51. The educational value of camera manipulation was 3.42 ± 0.67, instrument manipulation in small space 4.83 ± 0.39, and intracorporeal suturing and knot tying 4.83 ± 0.39. Overall satisfaction with the rubber plunger model was 5.0 ± 0.0 and no significant difference in scoring was found according to experience (4.31 ± 0.92 vs 4.33 ± 0.94, p=0.87).
Conclusion
The novel rubber plunger dry lab model for neonatal MIS training was successfully validated. Assessment demonstrated that this simulator is realistic and effective, particularly for practicing instrument handling and intracorporeal suturing in confined spaces. This provides a practical and ethical alternative to wet lab models.
Perioperative Support for Children Using Medical Clown Interventions: A Prospective Observational Survey of Healthcare Professionals
Abstract
Background
Preoperative anxiety affects a substantial proportion of children undergoing ambulatory surgery and may negatively influence perioperative cooperation and workflow. Non-pharmacological interventions, such as medical clowning, have been proposed to reduce anxiety; however, their integration into perioperative routines and interprofessional collaboration remains insufficiently explored from the perspective of healthcare professionals.
Aims
The aim of this study was to evaluate the quality of collaboration between medical clowns and hospital staff in the perioperative setting. Specifically, we sought to describe perceived effects, collaboration, and synergy associated with medical clown involvement, assessed qualitatively through satisfaction surveys filled by anesthesia team, recovery room nurses, and medical clowns.
Methods
A prospective monocentric observational study was conducted between February 2023 and October 2024. Pediatric patients aged 3–18 years scheduled for ambulatory surgery under general anesthesia were eligible. Medical clown interventions were delivered by trained professionals affiliated with a non-profit organisation. Satisfaction surveys were completed by operating room physicians and nurses, recovery room nurses, and medical clowns. Data were collected using a secure electronic data capture system and analysed descriptively, with a focus on collaboration and perceived impact on the patient and the perioperative healthcare professionals.
Results
A total of 139 consecutive pediatric patients were included. High satisfaction levels were reported across all professional groups. Medical clowns perceived a reduction in patient stress in 88–92% of cases and reported good integration without disruption of clinical care. Operating room and recovery room staff observed positive effects on patient mood in 82–85% of responses and reported smooth workflow integration. Interprofessional collaboration was consistently rated positively, supporting the feasibility of the intervention within routine perioperative practice.
Conclusion
Medical clown interventions were feasible and well accepted in the perioperative setting. Healthcare professionals reported positive collaboration and perceived benefits on patient mood without interference with clinical workflows. These findings support the potential role of medical clowning as a non-pharmacological adjunct to perioperative pediatric care.
Current Management of Isolated Pediatric Radial Neck Fractures: Results of a Multinational Survey
Abstract
Background
The management of isolated radial neck fractures in children relies on age-dependent remodelling potential and clinical judgement. However, contemporary treatment strategies across regions, healthcare systems, and surgical specialties remain insufficiently described.
Aims
The aim of this study was to evaluate current clinical practice patterns regarding indication thresholds, operative techniques, and aftercare of isolated paediatric radial neck fractures and to identify factors influencing decision-making.
Methods
An online survey was conducted among paediatric surgeons, paediatric orthopaedic surgeons, and trauma surgeons in Germany, Austria and Switzerland. Collected data included professional experience, angulation thresholds for reduction, operative techniques, aftercare, and awareness of institutional treatment thresholds. 111/116 responses provided at least one evaluable response and were included in the analysis.
Results
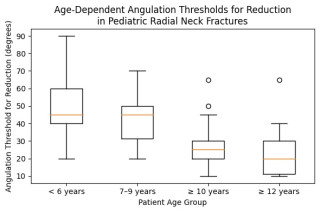
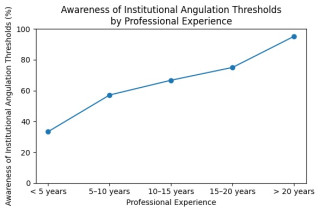
Median tolerated angulation thresholds decreased significantly with increasing patient age, from 45° in children younger than 6 years to 20° in children aged 12 years or older (Figure 1), while substantial inter-individual variability persisted across all age groups. Angulation thresholds did not differ significantly by country, surgical specialty, professional experience, hierarchical position, institutional level of care, or annual case volume. In contrast, awareness of institutional angulation thresholds was strongly associated with professional experience (Figure 2) and position, ranging from 33.3% in physicians with less than 5 years of experience to 95.2% in those with more than 20 years of experience (p < 0.01). Physicians aware of institutional thresholds more frequently performed radiographic follow-up and opted for shorter or no immobilisation following both operative and non-operative treatment. In cases of failed closed reduction, elastic stable intramedullary nailing (Metaizeau technique) was the preferred operative method (81% of respondents).
Conclusion
The management of isolated paediatric radial neck fractures demonstrates consistent age-dependent decision-making across regions and specialties but considerable individual variability, particularly in aftercare. Treatment differences appear to be driven more by professional experience and institutional knowledge than by regional or specialty-specific factors, underscoring the need for structured, age-adapted treatment recommendations and improved dissemination of institutional standards.
The Impostor Phenomenon in Pediatric Surgeons in Switzerland
Abstract
Background
Impostor Phenomenon (IP) is characterized by persistent self-doubt and the externalization of achievements despite objective evidence of competence. IP occurs more frequently among physicians, and it appears to be particularly prevalent among female surgeons. It is associated with an increased risk of burnout, as well as anxiety and job dissatisfaction. Pediatric surgery is a subspecialty with a significant number of female surgeons.
Aims
Our objective was to characterize IP within the Swiss pediatric surgery community.
Methods
In December of 2025, an electronic survey was distributed to all surgeons affiliated with the Swiss Pediatric Surgical Association and sent to all swiss pediatric surgery departments. The survey instrument incorporated two validated scales: the Clance IP Scale (CIPS) and the Copenhagen Burnout Inventory (CBI), and demographic data.
Results
75 people completed the questionnaire. 62,3% were female, 33% were between 40 and 49 years old. 20% were residents, 80% were trained pediatric surgeons. The median CIPS was 61 (IQR 45 to 73) indicating frequent IP signs. 24% stated that they are affected by IP, 88% of those were women. The CBI score indicates a low risk of burn out (score <50): personal CBI with mean 46 (IQR 33 to 64), work related 43 (IQR 29 to 54) and lowest in the patient related part with mean 16 (IQR 29 to 54). Female and younger respondents were more likely to suffer from higher IP (p<0.001) and burn out scores (P<0.05). There was a mild correlation between the CIPS and CBI (Pearson-Korrelation, p<0.001).
Conclusion
IP is a relevant Phenomenon among Swiss pediatric surgeons and is commonly associated with a risk for burn out. In our cohort, women had a higher risk for burn out and higher IP scores.The implementation of personal and system-level interventions are necessary to potentially mitigate the adverse effects of IP.
Introducing a coordinating physician in a pediatric surgery unit: impact on workflow and care coordination
Abstract
Background
Pediatric surgery units face clinical complexity, high turnover of junior doctors, and growing administrative burden, all of which may negatively affect continuity of care, patient/family satisfaction and efficiency. While physician-assistants/nurse-practitioners have shown to improve clinical continuity and workflow in adult surgical wards, their impact is less explored in pediatric surgical settings.
Aims
This study aimed to evaluate the perceived impact of introducing a coordinating physician (CP) in a pediatric surgery team on workflow metrics, care coordination and team functioning, from the perspective of interns and nurses.
Methods
A cross-sectional survey study was conducted in a tertiary pediatric surgery unit following the introduction of a CP. Two anonymous, self-administered questionnaires were distributed to two rotations of pediatric surgery interns (before/after CP-introduction) and to nursing staff. Items assessed administrative workload, continuity of care, efficiency and overall team functioning using Likert-scale responses. Descriptive analyses were performed.
Results
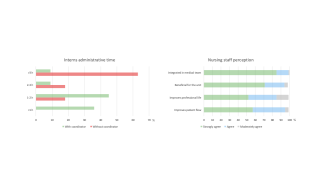
Among interns (n=12), the most frequently reported administrative challenges without a CP were scheduling patient appointments (75%) and follow-up/results retrieval (75%), followed by discharge paperwork (58%). Daily administrative time without a CP was estimated >3 hours in 63%, 2–3 hours in 18%, and 1–2 hours in 18%. With a CP, time decreased to 1–2 hours in 45%, <1 hour in 36%, 2–3 hours in 9%, and >3 hours in 9% (p=0.02). Perceived benefits included improved unit functioning (83% strongly agree), quality of work life (67% strongly agree), and patient pathway (75% strongly agree). System-wide implementation was supported by 83%.
Nursing staff responses (n=21) remained strongly positive (100% agreement for integration/benefit/patient flow; 81% earlier discharges) (Figure 1).
Conclusion
In this pediatric surgery setting, introducing a CP was associated with clearly perceived reductions in physicians’ administrative burden and improved discharge hours, strengthening the ward/team functioning and supporting a more patient-centered model of care delivery.
Intracerebral empyema as a rare complication of pediatric sinusitis: A case report
Abstract
Background
Sinusitis is a common condition in the pediatric population and is usually benign; however, in rare cases, it can lead to severe intracranial complications. This case report describes a rare presentation of complicated sinusitis with intracerebral empyema and highlights key diagnostic and therapeutic considerations to prevent this outcome.
Conclusion
This case highlights that intracerebral empyema is a rare but life-threatening complication of pediatric sinusitis, where timely recognition, prompt neuroimaging, and rapid interdisciplinary intervention are crucial for a favorable outcome.
Case presentation
We report on a previously healthy school-aged child admitted with fever, photophobia, and meningeal signs following chronic rhinosinusitis. Laboratory studies showed markedly elevated inflammatory markers. Contrast-enhanced MRI revealed pansinusitis with contiguous intracranial spread from the right frontal sinus, resulting in an intracerebral empyema. Emergency endoscopic sinus surgery and empirical broad-spectrum antibiotics were initiated and later tailored to microbiological results. Due to postoperative progression of the empyema, neurosurgical evacuation via osteoclastic craniectomy became necessary. Despite transient neurological complications, including seizures, the patient’s condition improved steadily under combined surgical and antibiotic therapy. He was discharged in good health, with no residual deficits, and follow-up imaging confirmed complete resolution.
Multidimensional Distal Radius Lengthening Osteotomy Following Posttraumatic Physeal Arrest in an Adolescent: A Case Report
Abstract
Background
Distal radius fractures account for nearly 40% of pediatric fractures, making them the most common fracture in childhood. Approximately 15–30% of these fractures involve the distal radial physis and may result in partial or complete growth arrest, potentially causing limb length discrepancies, angular deformities and functional impairment.
Conclusion
Although distal radius fractures are very common, posttraumatic physeal arrest in this region is rare but may result in clinically significant deformity, including ulnar-positive variance and wrist dysfunction. Multidimensional distal radius lengthening osteotomy combined with ulnar epiphysiodesis is an effective treatment option. Meticulous preoperative planning and patient-specific implants may further improve surgical accuracy and clinical outcomes.
Case presentation
A 13-year-old female athlete presented with progressive bony prominence of the ulnar styloid and load-dependent wrist pain. Clinical examination revealed protrusion of the ulnar styloid and moderate distal radioulnar joint instability with symmetrical ROM (range of motion).
Approximately one year prior, she sustained a distal radius fracture with suspected involvement of the distal radial physis, treated conservatively at an external clinic. Radiographs showed an incomplete posttraumatic physeal arrest, progressive multidimensional radial growth disturbance, and secondary ulnar-positive variance. Bilateral forearm CT revealed a 20 mm longitudinal discrepancy.
After meticulous virtual planning, a multidimensional distal radius lengthening osteotomy was performed using a custom-made palmar radius plate, corticocancellous iliac crest bone graft and permanent distal ulnar epiphysiodesis. Initial transient functional impairment and dysesthesia of all fingers were attributed to the achieved 16 mm radial lengthening. Immobilization in a forearm splint was maintained for six weeks, with load-free occupational hand therapy initiated after two weeks. Serial clinical and radiographic follow-ups demonstrated complete consolidation, regression of dysesthesia, and restoration of symmetrical wrist and finger ROM with full return to sports by five months postoperatively.
Ten Hot Topics in 6 Minutes
New Standard of Multimodal Treatment in Upper GI Cancer
Update on Medications for Weight Loss and Their Implications for Bariatric Surgery
Novel S3 Guideline on Well-Differentiated Thyroid Cancer – What’s New?
How Do the New ATA Guidelines Differ From the German Guidelines of Well-Differentiated Thyroid Cancer?
What’s the Role of Long-Term Absorbable Meshes in Hernia Surgery?
Is There Still a Role for Conservative Treatment in Acute Cholecystitis?
VacStent – Novel Indications in Colorectal Surgery- Can it Replace Stoma Placement?
Update on Pancreatitis Treatment – Guidelines 2025 – Is Stepup Still the Way to Go?
Update on Locoregional Non-Surgical Therapies of HCC
Immunotherapy of the GI Tract – Where Has It Advanced to First Line-Therapy?
Late Breaking: First Results of a Multicentre Randomised Controlled
Trial on Intraoperative Briefings (the StOP?-II Trial)
Do intraoperative briefings improve patient outcomes? A brief, structured exchange of information during the operation improves the team's situation awareness. The StOP?-II study has now tested whether this also affects patient mortality.
Thoracic Surgery - Free Comunication
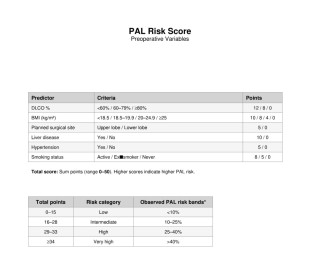
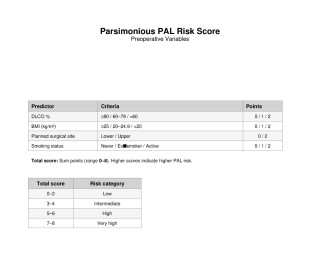
Development of a Preoperative Risk Score to Predict Prolonged Air Leak after Uniportal VATS Segmentectomy
Abstract
Background
Air leak (PAL) is the most common complication after segmentectomy and prolongs drainage and hospital stay. No bedside risk tool exists specifically for uniportal segmentectomy.
Aims
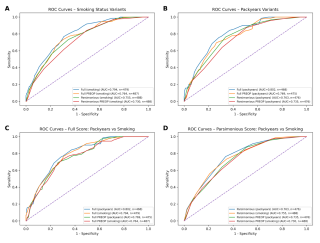
We developed point-based PAL risk scores derived from our primary analysis and evaluated both full and preoperative-only performance
Methods
We conducted a retrospective single-centre cohort study of consecutive uniportal VATS segmentectomies performed between 2015 and 2023. PAL was defined as an air leak lasting >5 days. Predictors were analyzed using logistic regression supported by elastic net modeling. Weighted and parsimonious point-based scores were derived including variants to preoperative variables. Smoking was modeled as pack-years or smoking status. Performance was assessed using AUC (bootstrap 95% CI), paired AUC comparisons, and calibration across risk strata.
Results
A total of 575 uniportal segmentectomies were included. Multivariable analysis identified upper lobe location, reduced diffusion capacity (lower DLCO%), low BMI, hypertension, liver disease, long surgery time, and additional wedge resection from another segment as independent predictors of PAL. Elastic net modeling confirmed these variables as the most informative, achieving ~70% classification accuracy and supporting translation into point-based scores. Using smoking status instead of pack-years, the weighted full score showed good discriminatory power (AUC 0.794). The parsimonious bedside score (0–2 points/item) achieved an AUC of 0.755. (Fig.1 and 2) Modeling smoking as pack-years provided only minimal improvement (ΔAUC ≈ +0.01). Restricting prediction to preoperative variables led to a modest reduction in performance (complete preoperative AUC 0.764; parsimonious preoperative AUC 0.730) approximately 0.03 AUC lower than the corresponding full models. (Fig.3) Observed PAL rates increased stepwise across risk categories, with good calibration and no major miscalibration in the intermediate-risk range.
Conclusion
We developed two clinically useful PAL risk scores for uniportal VATS segmentectomy with good discrimination (AUC ~0.73–0.80) and minimal sensitivity to smoking definition. Preoperative-only versions were prioritized for clinical decision-making. Prospective external validation and impact analysis are recommended.
Continuous Paravertebral Catheter vs. Single-Shot Intercostal Block: Optimizing Postoperative Analgesia in Thoracic Surgery
Abstract
Background
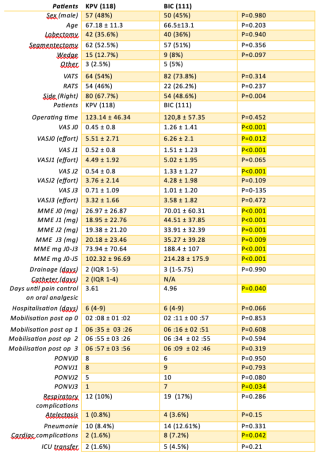
Effective regional analgesia plays a pivotal role in perioperative pain management by reducing opioid requirements and related complications, such as postoperative nausea, paralytic ileus, and impaired postoperative mobilization. Despite its importance, the optimal technique remains debated. This study compared the efficacy of continuous paravertebral catheter (KPV) versus single-shot intercostal block (BIC) in patients undergoing video-assisted (VATS) and robotic-assisted (RATS) lung resection.
Aims
To compare the efficacy of KPV against BIC in optimizing postoperative analgesia, reducing opioid consumption, and improving clinical recovery in thoracic surgery patients.
Methods
This prospective observational study (September 2024–November 2025) compared intraoperative KPV against BIC within a standardized multimodal protocol. Primary outcomes included Visual Analogue Scale (VAS) pain scores and cumulative opioid consumption (MME). Secondary outcomes included complications and time to oral analgesia. A 1:1 propensity score-matched analysis adjusted for baseline imbalances.
Results
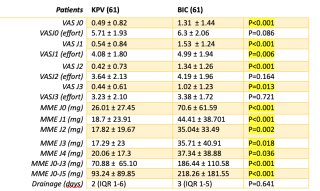
Of 229 patients undergoing lung resection (82 lobectomies, 119 segmentectomies, 24 wedge) via VATS or RATS, 118 received KPV and 111 BIC. KPV significantly reduced resting pain (POD 0-2) and opioid consumption (73.9 vs 188.4 mg MME, p < 0.001) over the first three days, differences persisting to day 5 (table1). In matched cohorts (61 patients/group, table 2), KPV provided superior resting analgesia (POD 0-3, P<0.001; P=0.013) and reduced pain on effort (POD 1, P=0.006). Cumulative opioid consumption (J0–J5) was significantly lower with KPV (93.2 vs 218.3 mg MME, P<0.001). KPV also facilitated earlier transition to oral analgesia (P=0.04) and was linked to fewer cardiac complications (P=0.042), despite 10.7% catheter dislocation.
Conclusion
Continuous paravertebral analgesia provides superior, sustained pain relief and profound opioid sparing compared to intercostal block, supporting its prioritization in enhanced recovery pathways despite a learning curve for catheter placement.
Abandoning Routine Chest X-Rays After Chest Tube Removal and Non-Anatomical Lung Resection? A Retrospective Cohort Study
Abstract
Background
Chest X-rays (CXR) after chest tube removal remain common after lung surgery, despite unclear clinical benefit and increased workload and can lead to unnecessary follow-up examinations. Previous studies show that routine CXRs rarely change management.
Aims
We evaluated the utility of post-removal CXR after minimally invasive wedge resection and predictors of clinically relevant pneumothorax
Methods
We conducted a retrospective, single-centre cohort study of consecutive patients undergoing minimally invasive wedge resection between January 2019 and December 2022. The primary endpoint was post-removal complications requiring intervention. Secondary endpoints included radiological findings, symptoms, and treatment changes after chest tube removal.
Results
A total of 189 patients were included; all underwent post-removal CXR. The cohort was predominantly male (66.1%), with high comorbidity (ASA 3-4: 82%); 20.1% had COPD, and 40.7% were active smokers. Median time to chest tube removal was 1 day [1–2] and median length of stay was 2 days [2–3]. Post-removal CXR was abnormal in 55.7% of the cohort, most commonly showing pleural effusion (41.3%) or pneumothorax (30.7%);
Among patients with pneumothorax (n=59), median size was 0.7 cm [0.5–1.2]; 25.9% of which were > 1 cm and 12.1% >2 cm. Symptoms occurred in 4.2% and were more frequent with pneumothorax (8.6% vs 2.3%; p=0.059). Treatment changes were necessary in 13.8%, mainly oxygen supplementation 11.6% of the whole cohort and were strongly linked to abnormal CXR (23.1% vs 1.2%) and pneumothorax (31.0% vs 6.1%)
Invasive interventions were rare (1.6%) and re-admission rate was 3.7% Treatment changes were more frequent with abnormal CXR findings 23.1% vs 1.2% (p <0.05) and pneumothorax (p<0.05). Adhesiolysis (OR 2.98, 95% CI 1.45–6.14) and lower BMI (OR 0.93/kg/m², 95% CI 0.88–1.00) independently predicted pneumothorax
Conclusion
Although post-removal CXR abnormalities were common, clinically relevant interventions were rare and limited to symptomatic patient. Selective imaging based on symptoms may safely replace routine CXR after wedge resection, particularly in low-risk patients.
Efficacy of Non-powered Stapler in Lung Volume Reduction Surgery of Severe Lung Emphysema: A Prospective Randomized Single-Blinded Monocentric Study
Abstract
Background
Lung volume reduction surgery removes diseased emphysematous tissue but is often complicated by postoperative air leaks. Using staplers helps seal lung edges; manual staplers rely on surgeon force, while powered staplers aim to minimise tissue trauma and lower air-leak risk. Few studies compare both in LVRS.
Aims
This study aimed to assess whether the use of the non-powered AEONTM Endostapler during lung resection in patients with severe lung emphysema reduces the duration of postoperative air leak, as measured by the air leak volume over time, in comparison to the Echelon FlexTM Powered Plus Stapler in a prospective, randomised setting.
Methods
A total of 32 LVRS were performed on 19 patients, stratified by side of the operation. These procedures were randomly assigned to utilize either the non-powered or the powered stapler. Postoperative air leak was monitored using a digital recording system. The time to air leak closure, the incidence, and severity of air leaks, as well as the duration of chest tube placement were evaluated.
Results
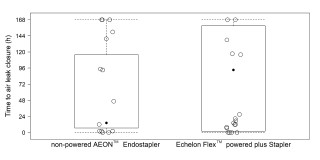
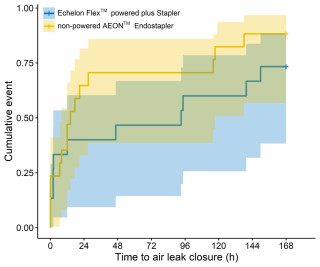
Immediate postoperative air leaks were observed in 6 of 17 procedures (35.3%) using the non-powered and in 9 of 15 procedures (60%) performed with the powered stapler. The median time to closure of the air leak was considerably shorter in the non-powered procedures: 14.3 hours [6.7, 116] compared to 93.2 hours [2.1, 159] for the powered treatments (Figure 1.). Cox regression analysis yielded a Hazard ratio of 1.6 (95% CI: 0.73-3.3) for a faster air leak closure with the non-powered stapler (P = 0.25) (Figure 2.).
Conclusion
Both stapler systems are feasible for use in patients with severe lung emphysema. However, our results suggest a potential advantage of the non-powered stapler, as earlier air leak closure was achieved with it.
Early detection of treatment relevant coronary arteriosclerosis within the lung cancer screening program
Abstract
Background
Smoking is a major cause of preventable morbidity and mortality worldwide and contributes to lung cancer, COPD, stroke, and coronary heart disease. Lung cancer remains the most lethal malignancy, with smoking as its principal etiologic factor, and early detection with low-dose computed tomography (LDCT) reduces mortality. Since 2019, a feasibility study on LDCT-based lung cancer screening (LCS) has been conducted at the University Hospital Zurich.
Aims
Because smoking is also a key risk factor for coronary atherosclerosis, this study aimed to evaluate the prevalence, severity, and clinical relevance of incidental coronary artery calcification (CAC) in LCS participants and to assess its associations with age and cumulative smoking exposure.
Methods
We retrospectively evaluated 201 current or former heavy smokers from the Swiss LCS feasibility study. CAC was visually scored using the SHEMESH method across four coronary arteries (0–3 per artery; total 0–12). Relationships between CAC, age, and pack-years were analyzed using a generalized linear mixed model. Participants with CAC >4 were referred for stress testing and followed for four years.
Results
CAC was detected in 55.7% (112/201): 30.8% mild, 15.9% moderate, and 8.9% severe. CAC correlated with both age (p=0.032, r=0.098) and pack-years (p=0.011, r=0.037). Among 50 participants with CAC >4, one was lost to follow-up, two excluded, 28 had negative stress tests, 8 remain under evaluation, eight (19.5%) had prior cardiac events, and three (6.3%) underwent coronary angioplasty with stent placement. Most calcifications involved the Left Anterior Descending artery and the Right Coronary artery. Nine participants reported exertional dyspnea or atypical chest pain.
Conclusion
Incidental CAC was prevalent and linked to age and cumulative smoking exposure. Identifying treatment relevant coronary arteriosclerosis requiring stenting in 6.3% of cases transforms LCS from passive risk stratification into a proactive intervention for myocardial infarction prevention.
Tumor Board vs. AI: Evaluating Concordance in Lung Cancer Treatment Decisions
Abstract
Background
Artificial intelligence (AI) is playing an increasingly relevant role in clinical decision-making, with the potential to support tumor board decisions in the future. However, the system is still in its developmental stages, and a practical understanding in lung cancer treatment decision-making is needed.
Aims
This study aims to provide an overview of how AI can assist in tumor board (TUB) decisions in lung cancer treatment.
Methods
The study considered patients diagnosed with non-small cell lung cancer during the first six months of 2025 at our lung cancer centre. Data was collected from TUB meetings prior to therapy start and after treatment initiation. Structured, pseudonymized clinical case summaries were provided as input, and AI outputs were compared with institutional TUB decisions. AI-generated treatment recommendations were obtained using ChatGPT (OpenAI, San Francisco, CA, USA), a commercially available generative AI model (GPT-4.1). The model was used without task-specific fine-tuning or retrieval-augmented generation.
Results
In this cohort of 64 patients with non-small cell lung cancer, all patients provided informed consent for further data processing. 30 were female (46.9%). Clinical tumor staging was as follows: 50 patients were staged I and II, 10 patients staged III and IV and 4 with multiple synchronous lung cancers. Surgical procedures included 34 lobectomies/bilobectomy, 24 segmentectomies, and 5 atypical resections.
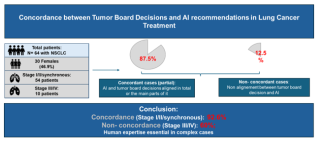
The concordance (and partial concordance) between TUB decisions and AI-generated recommendations was 92.6% (Stage I and II and synchronous). However, this was only the case for 60% in the advanced stages.
Conclusion
In this study, we observed that the concordance between TUB decisions and AI-generated recommendations was stage-dependent. This highlights the critical role of human expertise, where clinical judgment and the consideration of individual patient factors are dominant. To improve the system, we will further evaluate this approach in a larger cohort and, in a second step, incorporating deep machine learning techniques to refine and enhance the system's decision-making.
Salvage Surgery for NSCLC: Another Chance or a Risky Try? A Retrospective Study
Abstract
Background
Non-small cell lung cancer (NSCLC) remains the leading cause of cancer-related mortality worldwide. Although advanced disease has traditionally been treated with palliative intent, modern systemic therapies—immunotherapy, targeted agents, chemotherapy, and radiotherapy—have enabled improved tumor control in selected patients. This evolution has reopened discussion on the role of surgery within multimodal strategies for advanced stages. While planned surgery following neoadjuvant therapy is well established, value of salvage surgery for residual, persistent, or recurrent disease after systemic treatment remains poorly defined.
Aims
This cohort study aimed to assess the feasibility, safety, and oncological outcomes of salvage surgery, using surgery after neoadjuvant treatment as the most comparable clinical reference.
Methods
We performed a retrospective single-center analysis of patients with advanced NSCLC who underwent pulmonary resection between March 2021 and July 2024. Patients were divided into two groups: salvage surgery for residual or recurrent disease following systemic therapy and/or radiotherapy (n=11), and planned surgery after neoadjuvant treatment with curative intent (n=20). Surgical procedures, pathological outcomes, and postoperative morbidity were analyzed. Complications graded according to the Clavien–Dindo classification. Disease-free survival (DFS) and overall survival (OS) estimated using the Kaplan–Meier method.
Results
Patients undergoing salvage surgery presented with more advanced initial disease, including a higher proportion of metastatic stages. Lobectomy was the most frequent procedure in both groups. Complete resection (R0) was achieved in 90.9% of salvage surgeries and 100% of planned surgeries. Postoperative morbidity (Clavien–Dindo ≥2) was comparable (63.6% vs. 60%), with no 90-day mortality. At 24 months, DFS was approximately 50% in salvage group and 70% in other group. OS was 55–60% and 75%, respectively.
Conclusion
In carefully selected patients, salvage surgery for advanced NSCLC is feasible and safe, achieving high rates of complete resection with acceptable morbidity despite extensive pretreatment. Within experienced thoracic centers and multidisciplinary decision-making, salvage surgery represents a legitimate component of modern multimodal management.
Perioperative Outcomes after sublobar lung resection: The impact of anatomical location and resection complexity
Abstract
Background
Sublobar anatomical lung resection (SARL) is increasingly used for early-stage lung cancer and for patients with limited cardiopulmonary reserve. Although oncological results of segmentectomy are established, perioperative risk differences between specific SARL procedures remain unclear.
Aims
We assessed outcomes after SARL by anatomical location and extent of resection, and explored the impact of procedural complexity and 3D reconstruction.
Methods
This retrospective single-center study included all adults undergoing SARL between January 2015 and February 2023. Endpoints were 30-day and 90-day mortality, 30-day morbidity or readmission, blood loss, operative time (OT), and length of stay (LOS). Categorical variables were compared with chi-square or Fisher’s exact test and continuous variables with nonparametric methods.
Results
Overall, 573 patients were analyzed; 57.9% were male. Mean age was 65 ± 10 years and mean body mass index 25.2 ± 4.7 kg/m². Right-sided SARL had higher 30-day morbidity than left-sided resections (32.9% vs 24.7%, p = 0.032). Thirty-day mortality was identical (0.7% vs 0.7%), while 90-day mortality was numerically higher on the right (2.4% vs 1.4%) without significance. Median LOS was 3 days in both groups. Median blood loss tended to be higher on the right (150 vs 100 ml).
Overall 30-day mortality was 0.55% (n = 4) and 90-day mortality 1.65% (n = 9), with no significant differences across anatomical segments. In contrast, 30-day morbidity differed by segment (p < 0.001), with highest rates after right upper lobe single-segment resections (31.6%) and left upper lobe combined or multisegment resections (25.0%). LOS (p = 0.003) and OT (p = 0.019) also varied, with longest OT after right lower lobe combined resections and left lingular resections. Blood loss did not differ significantly overall.
Conclusion
Perioperative outcomes after SARL vary by location and extent. Mortality is low, but morbidity, OT, and LOS increase in more complex combined resections, supporting tailored planning and counseling overall.
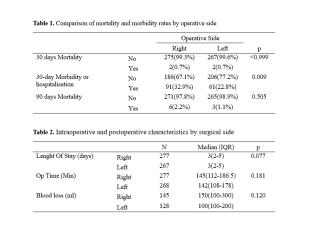
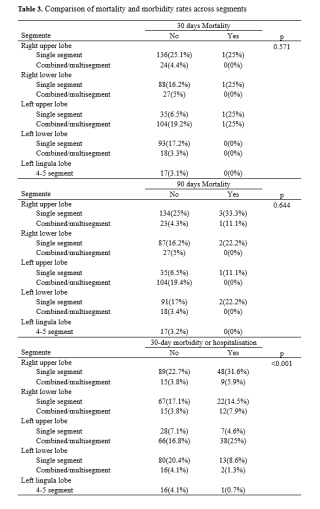
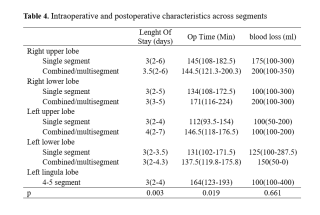
Vacuum Bell Therapy as a Non-Surgical Alternative for Pectus Excavatum: Real-World Experience
Abstract
Background
Pectus excavatum (PE) is the most common congenital anterior chest wall deformity and can lead to functional limitations and psychosocial distress. While surgical correction is standard for moderate to severe cases, vacuum bell therapy (VBT) has established itself as a non-invasive, alternative.
Aims
Despite the increasing use of VBT, high-quality evidence regarding its effectiveness, and predictors of success remains limited. This study aims to evaluate the outcomes, predictors of response, and safety profile.
Methods
We conducted a retrospective cohort study of patients with PE treated with VBT between January 2017 and August 2025. Longitudinal changes in PE depth were assessed using rod-scale measurements. Treatment success was defined as complete correction at the last follow-up (residual depth ≤0.5cm and >25% depth reduction). Predictors were assessed using multivariable regression; adverse events and adherence measures were recorded.
Results
The cohort included 118 patients (mean age 16.8 years), predominantly male. Mean pectus depth decreased from 2.02 to 1.52 cm, mean improvement of 23.3%. Complete correction was achieved in 7.6%, while 50.8% and 16.1% achieved improvements of >25% and 50% respectively.
Treatment response was heterogeneous and frequently non-linear over time. Longer treatment duration independently predicted a >25% improvement (OR 1.66 per doubling; p=0.003, 95% Cl, 1.19-2.31); higher suction pressure was also associated with improved outcomes (OR 1.55 per +0.05mbar; p=0.047, 95% Cl,1.01-2.39). Adverse events occurred in 22% of patients and were predominantly skin complications.
Conclusion
In this real-world cohort, VBT resulted in clinically significant improvement in approximately half of treated patients. Treatment response was heterogenous and strongly influenced by treatment duration, with chest wall morphology and suction pressure also contributing to outcomes. VBT was generally safe, with mostly mild adverse events. These findings support VBT as a reasonable conservative treatment option for motivated patients with mild-to-moderate PE, provided that realistic expectations, prolonged therapy, and adherence are incorporated into shared decision-making.
First Swiss Case of Controlled DCD Multi-Organ Procurement Using Abdominal Normothermic Regional Perfusion and OCS-Heart Preservation
Abstract
Background
Controlled donation after circulatory death (cDCD) has been increasingly adopted across Europe to expand the donor pool. Abdominal normothermic regional perfusion (A-NRP) restores oxygenated blood flow to abdominal organs after circulatory arrest, allowing functional assessment and mitigation of warm ischemic injury. In parallel, ex-situ normothermic heart preservation using the Organ Care System (OCS-Heart) has enabled heart transplantation following cDCD. However, the combination of abdominal NRP with ex-situ heart preservation during a single, fully coordinated multi-organ procurement remains uncommon and has not previously been reported in Switzerland.
Conclusion
This case demonstrates the feasibility of a complex, fully coordinated cDCD multi-organ procurement strategy combining abdominal normothermic regional perfusion with ex-situ heart preservation using OCS. To our knowledge, this represents the first Swiss case of multi-organ recovery, including heart, lungs, liver, and kidneys, from a cDCD donor using this combined approach, supporting further national development of advanced cDCD programs.
Case presentation
We report the case of a 45-year-old male donor who underwent controlled DCD (Maastricht III) following withdrawal of life-sustaining therapy for aneurysmal subarachnoid hemorrhage. The agonal phase lasted 23 minutes, followed by a 5-minute no-touch period. Abdominal NRP was initiated 13 minutes after circulatory arrest and maintained for 2 hours and 24 minutes. Hemodynamic stability and metabolic parameters progressively improved during A-NRP, with decreasing lactate levels and preserved urine output. One liter of oxygenated blood from the NRP circuit was used to prime the OCS-Heart system for ex-situ heart perfusion. The heart, lungs, liver, and both kidneys were successfully retrieved and transplanted.
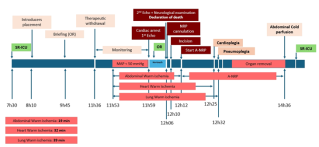

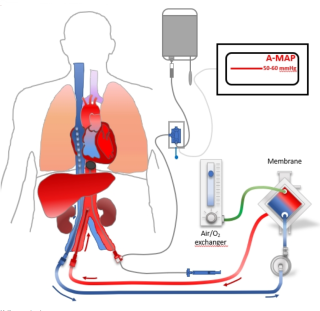
Primary Graft Dysfunction and Baseline Lung Allograft Dysfunction: Risk Factors and Associations With Outcomes After Lung Transplantation
Abstract
Background
Primary graft dysfunction (PGD) is the main cause of early morbidity and mortality after lung transplantation (LTx). Baseline lung allograft dysfunction (BLAD), indicating impaired graft function one year after LTx, is less well characterized, and its relationship with PGD remains uncertain.
Aims
We aimed to identify risk factors for PGD and assess its association with BLAD and outcomes.
Methods
All LTx recipients at Lausanne University Hospital (2008–2021) were retrospectively analyzed. Multivariate logistic regression identified risk factors for PGD and its association with BLAD and survival.
Results
Among 276 patients, 65 (23.6 %) developed PGD III. Independent predictors were younger age (OR 0.98/y, p = 0.025), female sex (OR 2.45, p = 0.003), lower donor PaO₂/FiO₂ (OR 0.99 per 10 mmHg, p = 0.02), and higher transfusions (OR 3.3, p < 0.01). PGD III was associated with prolonged ventilation (57 % vs 15 %, p < 0.01), reoperation (32 % vs 13 %, p < 0.01), longer ICU (22 vs 5 days, p < 0.001), and hospital stay (38 vs 24 days, p < 0.001). BLAD occurred more often in PGD III (59 % vs 38 %, OR 2.4, p = 0.009) and in patients transplanted for fibrotic lung disease (36 % vs 9 %, OR 5.8, p < 0.001). BLAD correlated with higher transfusions, reoperation, and prolonged ventilation. Survival did not differ between PGD III and non-PGD (1-, 3-, 5-y: 83.5 %, 74.2 %, 66.0 % vs 95.7 %, 87.1 %, 79.0 %; p = 0.53) nor between BLAD and non-BLAD.
Conclusion
PGD III after LTx is associated with increased perioperative morbidity and a higher risk of BLAD. Both conditions correlate with transfusion requirements and ventilatory complications, emphasizing the need for targeted perioperative strategies to improve graft recovery and long-term function.
Quality of life: An analysis of treatments for chronic thromboembolic pulmonary hypertension
Abstract
Background
Chronic thromboembolic pulmonary hypertension (CTEPH) can lead to drastically reduced quality of life (QoL). Pulmonary Endarterectomy (PEA) is the gold standard therapy for accessible lesions. For inoperable patients Balloon Pulmonary Angioplasty (BPA) serves as second line treatment. Efficacy of both treatments has been shown, yet data on the impact on QoL is widely missing.
Aims
We investigated changes in QoL for patients undergoing PEA or BPA.
Methods
CTEPH patients undergoing PEA or BPA in our institution between 2020-2025 were retrospectively analyzed. A validated QoL questionnaire (emPHasis-10) was used to assess health-related QoL before and one year after treatment. QoL data was compared with hemodynamic and clinical parameters such as reduction in mean pulmonary artery pressure (mPAP) and improvement of NYHA-class.
Results
62 patients receiving either PEA or BPA were analyzed. In the PEA group, mPAP improved by 20mmHg and emPHasis-10 by 13 points. In the BPA group (median of 3 BPA-sessions) mPAP improved by 10.5mmHg and emPHasis-10 by 3 points. NYHA improved by 1 class for PEA and stayed unchanged for BPA. At baseline both the PEA and BPA group had a median NYHA-class of 3. Paired Wilcoxon test showed an improvement in QoL for PEA patients (p<0.001). We report a reduction in mPAP in both PEA (p=0.001) and BPA (p=0.019) patients. Intergroup comparison showed larger hemodynamical improvement in PEA than BPA (p=0.009) and a significant change of QoL between the two groups (p=0.030). Pooling analysis for PEA and BPA patients showed concordant changes, hence bigger mPAP reductions correlate with bigger improvements in QoL.
Conclusion
Both PEA and BPA were associated with improvements in NYHA functional class and mPAP, with a greater reduction in mPAP observed after PEA. Improvements in quality of life were significantly higher in patients undergoing PEA. Overall, hemodynamic improvements were consistent with patients’ perceived gains in quality of life.
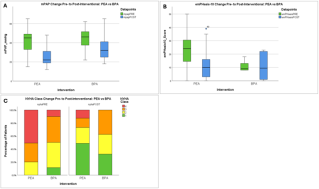
Young Vascular Medicine

Update of the New Vascular Surgery Training Program
Hot Topics – Vascular Emergencies
Impact of Vascular Diseases on Health Care Systems, From Carotis to Diabetic Foot
Work-Life Balance in Vascular Surgery CH – Results 2026
Simulators for Vascular Surgery Trainees
Early Start into Vascular Surgery
Coffee Break
AI, CAR T Cells and Omics in the OR: Will the Surgeons Still Be There?
AI in the OR
Immunotherapy and CAR T Cells: Will Surgery Still Be Necessary to Treat Cancer?
Organ Perfusion and Regeneration
Successful and Failed Liver Regeneration
From Barriers to Bridges: Rethinking Surgical Perspectives
Structural Barriers: Cutting Through Old Braids
Language as a Surgical Tool
Having it All: Living a Dream or Facing a Nightmare?
Discussion
Geriatric Fractures of the Proximal Humerus
Brief Overview of Demographic Challenge, Treatment Dilemma, and Session Format
Nonoperative Management – Why Less Is More
Osteosynthesis – The More, the Better
Primary Reverse Arthroplasty – The Gold Standard?
Conservative, Fix or Replace? A Case-Based Discussion
Joining Forces – What Can We Learn From Others
Congenital Intestinal Malformations
Iatrogenic Vascular Injury, I Need Your Help
Iatrogenic Ureteral Injury, What Now?
The Pregnant Patient: Tocolysis? What Medication to Give?
What We Can Learn From a Senior Surgeon
Joining Forces in Vascular Surgery
Urology–Vascular Collaboration in Oncologic and Reconstructive Surgery
Integrating Visceral and Vascular Expertise in Advanced Abdominal Surgery
Trauma and Vascular Challenges: Joint Approaches to Limb- and Life-Saving Surgery
Reconstruction in Sarcoma Surgery: A Multidisciplinary Imperative
Thoracic Surgical Perspectives in the Management of Thoracic Outlet Syndrome
Revascularization and Reconstruction: Coordinating Multidisciplinary Pathways for the Diabetic Limb – a Diabetologist’s Perspective
Joining Forces With Technology
From Concept to Competence in RATS: The French Robotic Lobectomy Training Blueprint
Introducing a Robotic Surgery Program in Thoracic Surgery – From VATS to RATS
A New Approach to Thymic Tumors – Redefining Surgical Strategy in the Robotic Era (Single-Port Approach)
Robotic Thoracic Outlet Surgery and Other Rare Indications in RATS
Two Decades of Robotic Thoracic Surgery at USZ: From Console Surgery to Robotic Navigation Bronchoscopy
Discussion
OR TEAM: Joining Forces Every Day! - Zusammenarbeit im Operationssaal stärken
This session is in German, but the session will be translated by an AI translation app. Bring your smartphone and headphones to experience the translation.


Einführung: Ziele und Ablauf OP-Team-Tag und Sitzung
Herausforderungen im Operationssaal – Die Perspektive der OP-Pflege
Sicht auf das OP-Team von der anderen Seite des Vorhanges - Die anästhesiologische Perspektive
Kommunikation, Lärm und Ablenkung im OP – Die wissenschaftliche Perspektive
Resiliente Operationsteams – Wie schaffen wir das?
Herausforderungen im OP gemeinsam meistern – Diskussionsrunde mit den Referentinnen und Referenten
Prix NaCHwuchs
Joining Forces for Pediatric Surgery Research
Adapting a clinical-grade decellularized esophagus for pediatric applications: pre-clinical evaluation in a minipig model.
Abstract
Background
The surgical management of Long-Gap Esophageal Atresia (LGEA) and esophageal strictures refractory to dilatation remains a major challenge, often requiring organ interposition (stomach, colon) associated with significant long-term morbidity. Tissue engineering offers a promising alternative to organ replacement. Recently, Saint-Louis Hospital (Paris) has successfully developed a clinical-grade decellularized esophageal scaffold, approved for adult trials (ESOGRAFT NCT06662370).
Aims
This preclinical study aims to assess the safety and efficacy of circumferential esophageal replacement using a decellularized adult porcine esophagus, remodeled for pediatric indications, in a minipig model.
Methods
Adult porcine esophagus are decellularized using the protocol established by the Cell Therapy Unit at St-Louis Hospital. To address pediatric anatomical constraints, adult scaffolds are remodeled ex-vivo to reduce their caliber (diameter: 10mm; length: 4cm) to match the pediatric esophagus. The study design involves 8 Yucatan minipigs aged of 2 months. The protocol consists of circumferential esophageal replacement protected by an omental wrap and a removable stent (maintained for 3 months). Animals are monitored for 6 months to assess clinical tolerance, nutritional autonomy, and weight gain. Post-mortem analysis focuses on structural remodeling, epithelialization (histology H&E), muscular regeneration, vascularization and neural pathways (immunohistochemistry).
Results
In-vivo evaluation is currently ongoing to assess long-term tissue remodeling at 6 months.
Conclusion
This study represents a critical translational step, trying to bridge the gap between adult clinical achievements and pediatric needs. By validating the downsizing of a clinical-grade scaffold in a relevant animal model, we aim to provide a safe solution for children with complex esophageal defects, avoiding the morbidity of autologous replacements.
Outcomes After Liver Transplantation in Sarcopenic Children: A Retrospective Analysis
Abstract
Background
Data on the impact of sarcopenia are limited in pediatric liver transplantation (LT). In contrast, sarcopenia has been extensively studied in adult LT recipients and has been shown to be associated with increased postoperative morbidity and mortality.
Aims
To evaluate the incidence and postoperative impact of sarcopenia in children having undergone LT.
Methods
This retrospective review included children (0-16 years) with LT, from 2004-2023. They were divided into two groups: sarcopenic vs non-sarcopenic patients, according to the Total Skeletal Muscle Index (TSMI)-score calculated on preoperative CT (with median TSMI-score in the second quintile as cut-off). Children with multi-organ transplants were excluded. Preoperative variables and postoperative complications during the first year post-LT were compared between the two groups.
Results
One hundred eleven patients were included, 78/111 (70%) were sarcopenic, 33/111 (30%) were not. Median TSMI-score was 2244 mm2/m2 (IQR 1984-2464). At LT, 75/111 patients (68%) received nutritional support, including 24/33 (73%) sarcopenic patients. Lower weight z-scores (p=0.03) and lower BMI (p<0.001) significantly correlated with sarcopenia. ICU length of stay was significantly longer in sarcopenic patients (p=0.035), whereas postoperative intubation time and overall hospital-stay did not differ between groups. Vascular, intestinal, biliary, infectious, neurological postoperative complications, and rate of reoperations were not significantly different between groups. In contrast, graft rejection during the first year post-LT was significantly associated with sarcopenia (p=0.003). Patient and graft survival did not differ between groups.
Conclusion
In this cohort of liver-transplanted children, sarcopenia was associated with prolonged ICU-stay and increased graft rejection within the first year post-LT. Interestingly and in contrast to adult series, surgical and infectious postoperative complications did not differ between groups. Further studies are needed to determine whether preoperative nutritional optimization, physiological resilience, or enhanced postoperative care might mitigate the clinical impact of sarcopenia in pediatric LT recipients.
Epidemiology of Necrotizing Enterocolitis in Multiple Birth Preterm Infants in Switzerland
Abstract
Background
Necrotizing enterocolitis (NEC) is a major cause of morbidity and mortality in preterm infants. Data comparing NEC incidence and outcomes between multiple birth and singleton preterm infants remains limited.
Aims
To report the incidence and mortality of NEC in preterm multiple-birth infants in Switzerland and to determine whether multiplicity independently contributes to NEC risk.
Methods
This is a retrospective cohort study analyzing data from the Swiss Neonatal Network collected between 2000 and 2021. A total of 16,411 preterm infants born at <32 weeks of gestational age were included, representing more than 95% of all Swiss preterm infants in this gestational age group (Figure I). Proven NEC cases, defined as Bell stage II or higher, were analyzed. NEC incidence and NEC-related mortality were compared between singleton and multiple birth preterm infants.
Results
32.5% of the population consisted of infants from multiple births (5,330/16,411)(Figure I). The overall NEC incidence was low (2.7%). NEC incidence was comparable between singleton and multiple birth infants (2.8% vs. 2.6%). NEC-related mortality did not differ significantly between groups, (39.3%) in multiple births compared to (33.7%) in singletons (Figure II). In twin pairs, the risk of NEC in the second twin was sixfold higher if the first twin was affected (OR 6.1 (CI 95% 2.4 - 16.2)).
Conclusion
The overall incidence of NEC in Swiss preterm infants is comparatively low. No relevant differences in NEC incidence or mortality were observed between multiple birth and singleton preterm infants. However, there is an increased risk of NEC in the second twin following an affected first twin. This suggests shared environmental or biological risk factors within twin pairs and highlights the need for vigilant monitoring of co-twins following NEC diagnosis in one sibling.
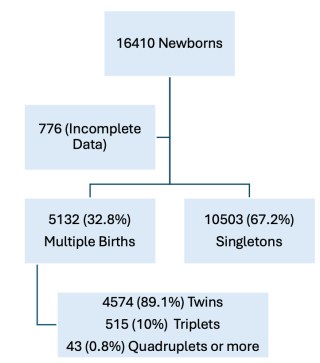
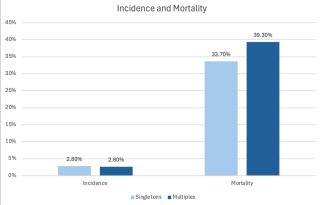
Multidimensional long-term outcomes after pediatric esophageal replacement following caustic injuries: A comparative study of two techniques.
Abstract
Background
Accidental ingestion of caustic substances is a significant pediatric health concern, potentially causing severe long-term gastrointestinal, nutritional, and psychosocial consequences.
Aims
This study aims to compare multidimensional long-term outcomes between children who underwent colonic pedicled flap versus gastric tube esophageal replacement in the mediastinum after caustic injuries.
Methods
This cross-sectional observational study was conducted during 2023-2024 in Benin and Togo through a Swiss-African surgical collaboration. Patients were operated on during their childhood between 1989 and 2022. They completed a comprehensive assessment using validated tools: Pediatric Quality of Life Inventory™ Gastrointestinal Symptoms Scale (PedsQL GI), KIDSCREEN-52 for psychosocial dimensions, SF-36 for general health perceptions, the International Dysphagia Diet Standardization Initiative (IDDSI) scale for dietary adaptation, and the Six-Minute Walk Test (6MWT) with the modified Borg scale for physical capacity.
Results
26 patients (aged 6–22 years, mean 14 years) were included. Among them, 17 had a colonic pedicled flap and nine a gastric tube. The mean operation-to-questionnaire interval was 8 years. No significant differences were observed between both groups in PedsQL GI, SF-36, or 6MWT outcomes. Mean PedsQL GI scores indicated mild-to-moderate gastrointestinal symptoms (lowest scores in 'Trouble swallowing': colonic 71 vs. gastric 69; 'Heartburn and reflux': colonic 75 vs. gastric 63). Significant psychosocial disparities emerged in KIDSCREEN-52, notably higher scores in Psychological Well-being (p<0.05) for colonic patients. Dietary texture modifications were needed in 38% of patients (IDDSI levels 5 and 6), equally distributed between groups.
Conclusion
Both colonic and gastric esophageal replacements provide satisfactory long-term functional outcomes with subtle psychosocial differences. Persistent dietary adaptations and gastrointestinal symptoms underline the necessity of tailored, multidisciplinary, and culturally sensitive follow-up.
Rescue Surgery in Acute Care: When and How to Intervene

Introduction & Session Objectives
Recognizing and Managing Anastomotic Leak After Elective GI Surgery
Postoperative Hemorrhage: When to Return to the OR?
Rescue Management of Surgical Site Infections and Wound Dehiscence
Rescue Strategies for Postoperative Respiratory Failure
Robotics – What We Need and Where We Are?
What Can We Learn From the US System?
Da Vinci SP
Da Vinci Xi (5)
Dexter
Hugo
Discussion Panel
Lunch
No Knots, More Speed: Maximizing Surgical Efficiency with Barbed Sutures
Sharing expertise with experts and hands-on training
Expert exchange in a relaxed atmosphere at the B. Braun Medical booth
Tutor: Joanna Janczak, Wil

Modern Leadership in Surgery
Eulogy of Honorary Member Prof. Dr. med. Markus Furrer
Principles of Systemic Leadership for Teams and Organizations
Mentorship for Trainees, Experiences of the Royal College of Surgeons
How to Lead a Symphony Orchestra
Colon
Gut Microbiota and Anastomotic Leakage in Colorectal Surgery: A Systematic Review.
Abstract
Background
Anastomotic leakage (AL) is a serious and potentially life-threatening complication following colorectal surgery, associated with increased morbidity, mortality, and impaired oncologic outcomes. Growing evidence suggests that the gut microbiome influences anastomotic healing and may represent a modifiable risk factor for AL. However, existing studies report inconsistent results, and no systematic review has yet comprehensively evaluated the association between gut microbiota and AL in clinical and experimental settings.
Aims
This study aims to systematically review the existing literature on the relationship between gut microbiota composition and the incidence of colorectal anastomotic leakage. Primary outcome was the incidence of anastomotic leakage. Secondary outcomes included microbial diversity, taxonomic signatures, histological or molecular markers of healing, and effects of microbiota-targeted interventions.
Methods
A systematic search of Medline, Embase, Web of Science, and the Cochrane Library was performed by three reviewers from inception to July 2025 following PRISMA 2020 guidelines. Randomized trials, cohort, and case-control studies assessing associations between AL and gut microbiota were included. Risk of bias was evaluated using ROBINS-I for non-randomized clinical studies and SYRCLE for preclinical studies.
Results
Twelve studies were included. AL was consistently associated with reduced microbial diversity and enrichment of pro-inflammatory or collagen-degrading taxa. In contrast, protective commensal bacteria were reduced. Several studies identified perioperative microbial signatures predictive of anastomotic healing or leakage. The C-seal device appeared to reduce microbiota differences between AL and non-AL patients.
Conclusion
Alterations in the gut microbiome are associated with impaired colorectal anastomotic healing. These findings support the role of microbiome-based risk stratification and perioperative interventions to reduce AL. A better understanding of microbial contributions may prompt a re-evaluation of current perioperative protocols, balancing infection prevention with preservation of beneficial commensal bacteria. Ultimately, microbiome-targeted therapies could emerge as adjuncts to enhance anastomotic integrity and reduce postoperative morbidity.
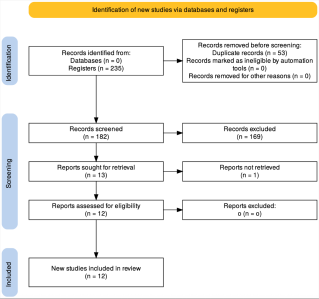
Is the Requirement to Remove Only 12 Lymph Nodes in Colon Cancer Surgery Still Justifiable?
Abstract
Background
Current guidelines consider the removal of ≥ 12 lymph nodes (LN) sufficient for accurate staging in colon cancer (CC). While the number of removed LN (RLN) severely depends on the quality of complete mesocolic excision and the pathological processing techniques, most European studies show a noticeably higher amount of RLN. Some recent studies have shown better survival in patients with ≥ 20 RLN, while others argue against due to higher complication rates.
Aims
We aimed to evaluate the prognostic impact of the number of RLN in CC and correlate the occurrence of postoperative complications.
Methods
This is a unicentre retrospective cohort study. We included all patients undergoing surgical resection for CC between 2014 and 2022 in a specialised centre in Switzerland. We defined four groups of RLN (<20, 20-25, 25-30 and >30) to analyse survival and complication rates. Survival rates according to the number of RLN were analysed using uni- and multivariate Cox regression.
Results
335 patients were included. The median number of RLN was 32. The four LN groups did not show any difference regarding UICC stage (p = 0.190). 5-year overall survival (OS) was significantly better in the groups with ≥ 20 RLN with 70% versus 45% in < 20 RLN (p = 0.044). In total, 8/335 patients showed anastomotic leakage (2.3%). Overall postoperative complications according to Clavien Dindo did not occur more frequently with increasing number of RLN (p = 0.88). Equally, specific complications like anastomotic leakage (p= 0.28), postoperative ileus (p = 0.47) and abdominal wound dehiscence (p = 0.89) did not show significant differences.
Conclusion
Our results demonstrate significantly better OS if ≥ 20 LN are removed in CC patients without higher complications rates regarding the number of RLN. Therefore, international guidelines should recommend the removal of ≥ 20 LN.
Laparoscopic Versus Robotic Right Colectomy: A Two-Year Comparative Outcome Analysis From a Single High-Volume Center
Abstract
Background
Minimally invasive approaches have become standard in colorectal surgery, with laparoscopic and robotic-assisted techniques associated with reduced postoperative pain, accelerated recovery, and shorter hospitalization. Laparoscopy has been established for several decades, whereas robotic surgery is increasingly adopted due to enhanced instrument articulation, improved ergonomics, and three-dimensional visualization. This study aimed to compare perioperative and postoperative outcomes of robotic (rRC) versus laparoscopic (lapRC) right colectomy.
Aims
A single-center cohort analysis of a prospectively maintained database was performed, including all patients undergoing elective right colectomy for malignant disease between January 2023 and January 2025. Patients were stratified according to operative approach (lapRC vs. rRC). Continuous variables were evaluated using independent t-tests and categorical variables using Fisher’s exact test. Statistical significance was defined as p<0.05.
Methods
A single-center cohort analysis of a prospectively maintained database was performed, including all patients undergoing elective right colectomy for malignant disease between January 2023 and January 2025. Patients were stratified according to operative approach (lapRC vs. rRC). Continuous variables were evaluated using independent t-tests and categorical variables using Fisher’s exact test. Statistical significance was defined as p<0.05.
Results
In total, 159 patients met inclusion criteria (lapRC n=89; rRC n=70). Mean operative duration was significantly longer in the rRC group (298 min; SD 103.82) compared with lapRC (218 min; SD 72.42; p<0.001). Conversely, conversion to open surgery was markedly lower following rRC (1.4% vs. 18%; p<0.001). Length of stay was shorter in the rRC cohort (7.6 vs. 11.6 days), although this difference did not reach statistical significance (p=0.303). Postoperative morbidity, quantified using the Comprehensive Complication Index, demonstrated no significant differences (rRC 7.8 vs. lapRC 9.1; p=0.5813), and anastomotic leak rates were comparable (2.9% vs. 4.5%; p=0.695).
Conclusion
Robotic right colectomy appears to reduce conversion to open surgery relative to conventional laparoscopy but is associated with prolonged operative time. Postoperative recovery profiles and complication rates were similar, suggesting that robotic-assisted right colectomy is a safe and viable minimally invasive alternative. These findings support the expanding integration of robotic platforms in colorectal surgery. However, randomized controlled trials are needed to validate oncologic equivalence, assess long-term functional outcomes, and determine cost-effectiveness.
Benchmarking-based audits as a quality improvement tool in minimal-invasive right hemicolectomies – experience from a single-centre analysis
Abstract
Background
Benchmarking enables objective comparison of institutional outcomes with reference benchmarks, derived from high-volume expert centers. Although benchmark values exist for multiple procedures and establishment used a standardized process, a structured methodological framework for comparing institutional data with benchmarks and for initiating quality improvement cycles has only recently been published but has not yet been evaluated for minimally-invasive right hemicolectomy (mis-RHC).
Aims
To assess the feasibility and value of a benchmark-based audit framework for mis- RHC and to identify potential areas for quality improvement.
Methods
All patients who underwent elective mis-RHC for adenocarcinoma between 2020-2024 at our institution were retrospectively analyzed. Inclusion and exclusion criteria followed the published benchmark study. Patients were classified as ideal or non-ideal. Evaluated parameters included operative time, conversion rate, length of hospital stay, lymph node yield, anastomotic leakage, severe complications (Clavien–Dindo ≥ IIIa), and readmission rate. Outcomes were analyzed in overlapping 18-month periods with 6-month intervals and compared with benchmark thresholds.
Results
Sixty-one patients met the inclusion criteria (ideal n=10, non-ideal n=51). In ideal patients, all resections were R0, lymph node yield exceeded benchmark values, and no conversions occurred. Operative time consistently exceeded benchmark limits, likely reflecting the teaching environment of a university hospital. Non-ideal patients were also compared against benchmarks defined for ideal patients; while this requires cautious interpretation, it revealed optimization potential mainly in postoperative processes and discharge management while oncological quality, reflected by R0 resection rate and lymph node yield, remained consistently above benchmark levels.
Conclusion
Benchmarking of mis-RHC provided meaningful insights into institutional performance. Deviations from benchmarks were thoroughly discussed in the team and attributable to patient characteristics or the academic training setting rather than structural quality deficits. This study demonstrates the applicability of benchmark-based audits for RHC and highlights their potential as a tool for continuous surgical quality improvement.
Safety and Feasibility of Ambulatory and Early Discharge Colectomy: A Systematic Review and Meta-analysis
Abstract
Background
Ambulatory and early discharge pathways after colectomy are gaining interest for resource optimization, although evidence regarding safety, feasibility, and outcomes is heterogeneous.
Aims
The aim of this study was to assess the safety of ambulatory and early discharge colectomy and optimal feasibility pathway.
Methods
A systematic review and meta-analysis was conducted following PRISMA guidelines. A comprehensive search of major bibliographic databases identified studies evaluating ambulatory or short stay colectomy. The primary outcome was 30-day hospital readmission. Secondary outcomes included postoperative complications, reoperation, mortality, length of hospital stay (LOS), and healthcare costs. Comparative analyses were performed between early discharge and inpatient cohorts when data were available.
Results
A total of 41 studies were included in the qualitative synthesis, and 37 studies comprising 191,898 patients were included in the quantitative analysis. Successful early discharge was achieved in 1,290 of 3,006 patients (42.9%). Overall readmission occurred in 7,308 of 140,139 patients (5.24%). Readmission rates were comparable between patients discharged within 24 hours and inpatients (4.62% vs 5.21%; OR 0.83, 95% CI 0.63–1.09), with no clinically relevant increase associated with early discharge. Postoperative mortality was low (0.1%) and did not differ between groups. Reoperation (1.2%), surgical site infection (2.2%), and postoperative ileus (2.1%) rates were infrequently reported but remained low overall. LOS was significantly shorter in the early discharge group (0.8 ± 0.4 vs 3.8 ± 2.7 days). Economic analyses consistently demonstrated lower costs associated with early discharge pathways, with a crude weighted saving of USD 5,809 per patient.
Conclusion
In carefully selected patients, ambulatory and early discharge colectomy appears safe and feasible, with readmission, reoperation, and mortality rates comparable to standard inpatient management, alongside a marked reduction in LOS and substantial cost savings. These findings support the implementation of structured early discharge pathways in selected populations, while emphasizing the importance of patient selection and postoperative surveillance.
Elective Ileostomy Reversal in Switzerland: A Nationwide Survey of Surgical and Perioperative Practices.
Abstract
Background
Elective loop ileostomy reversal is a common procedure, yet perioperative management remains poorly standardized and national data are lacking.
Aims
We aimed to describe current Swiss practices regarding preoperative assessment, operative technique, and postoperative management of elective ileostomy closure.
Methods
We conducted a nationwide, cross-sectional, web-based survey with one invitation and one reminder among members of the Swiss Society of Surgery between July and September 2025. Board-certified surgeons practicing in Switzerland who completed the full questionnaire were included. The survey addressed surgeon characteristics, preoperative work-up, technical aspects and postoperative care. Results are reported descriptively as numbers and percentages.
Results
102 board-certified surgeons were included. Most respondents practiced predominantly in the German-speaking region of Switzerland (76%). Most respondents were male (80%) and worked primarily in cantonal hospitals (34%). Annual experience with ileostomy reversal was limited: 57% reported performing 1–10 procedures per year. Preoperative assessment of the distal anastomosis was heterogeneous: 49% of surgeons routinely performed endoscopic evaluation and 44% used water-soluble contrast studies. Antibiotic prophylaxis was administered by 87% of respondents. The preferred anastomotic technique was hand-sewn end-to-end (55%), followed by latero-lateral configurations (hand-sewn or double-stapled). Mesh reinforcement was rarely used (1%). Skin closure was evenly distributed between linear closure (50%) and purse-string techniques (44%). Postoperatively, 71% recommended an unrestricted diet and 19% prescribed routine medications to stimulate bowel function. Discharge decisions were predominantly based on clinical recovery, most commonly passage of stool or flatus (33%) and tolerance of oral intake (33%).
Conclusion
This nationwide survey demonstrates substantial variability in the perioperative management of elective ileostomy reversal in Switzerland. While antibiotic prophylaxis and clinically driven discharge criteria are widely adopted, considerable heterogeneity persists regarding preoperative assessment and technical aspects of reconstruction. These findings highlight the need for evidence-based recommendations and provide a foundation for future consensus.
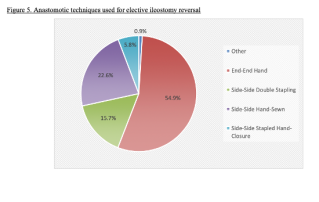
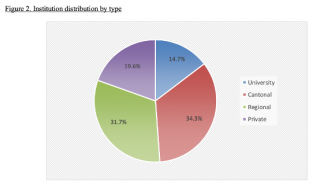
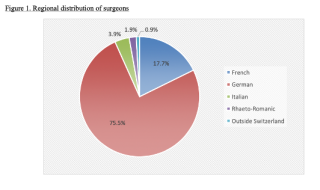
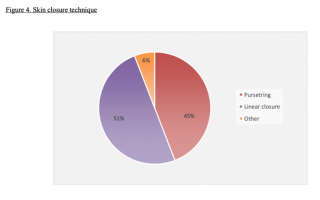
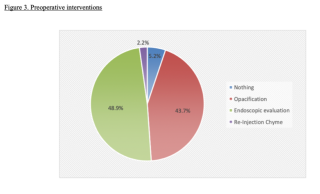
A decade of technical progress in the surgical treatment of ulcerative colitis
Abstract
Background
Despite an increasing number of medical options for the conservative treatment of ulcerative colitis (UC), surgery remains a cornerstone of therapy.
Aims
The aim of this study was to analyse temporal trends in colorectal surgery for ulcerative colitis, with particular focus on surgical indications, operative procedures, and perioperative outcomes.
Methods
Retrospective study including all patients with UC who underwent colorectal surgery at a tertiary referral centre between 2014-2024. Demographic data, surgical indications, operative procedures, and perioperative outcomes were analysed to assess temporal trends, with a focus on minimally invasive and robotic approaches.
Results
Fifty-nine patients were operated for UC. Colectomies as first surgery in a three-step procedure were performed in 42 patients (median age 35.6 (IQR 26.1; 46.6)) after a median of 5.9 years (IQR 2.7; 12.4) after diagnosis. Dysplasia was the indication for surgery in 3 patients, while 4 had colon cancer. 95% of colectomies were performed laparoscopically. Proctectomy and ileum pouch anal anastomosis (IPAA) was performed in 47 patients during the study period, a median of 210 days (IQR 184; 254) after colectomy. The proportion of robotic procedures increased substantially from 2017 onward, reaching 83.3% in 2024, without any detectable decline in quality during the implementation phase; notably, the last laparoscopic completion proctectomy/IPAA was performed in 2018. An elective two-stage procedure was performed in 12 patients mainly for dysplasia or rectal cancer (n=3) (median age 54.9 years (IQR 48.2; 59.2)) and a median of 20.6 years (IQR 15.7; 32.8).
Additionally, five patients were treated a median of 14 years after mostly ileorectal anastomosis for UC-associated rectal cancer and one rectal cuff cancer with poor prognosis and difficulty in preoperative diagnosis and staging.
Conclusion
Surgical management of ulcerative colitis at a tertiary referral centre has shifted toward predominantly minimally invasive and robotic approaches, with clear differentiation between acute disease-driven staged procedures and elective oncologic resections reflecting long-term disease burden.
Robotic-assisted CRS and HIPEC in Pseudomyxoma Peritonei: Case Report and Video Demonstration
Abstract
Background
Pseudomyxoma peritonei (PMP) is a rare malignancy characterized by mucinous ascites, often originating from perforated low-grade appendiceal mucinous neoplasms (LAMN). Disease progression causes abdominal distension, intestinal obstruction, and potentially fatal outcomes. Cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) represents the current standard treatment, offering potential long-term survival. However, these procedures are technically demanding, associated with substantial perioperative morbidity, requiring considerable expertise. Interest in minimally invasive, including robotic-assisted, approaches for selected patients with a low peritoneal cancer index (PCI) is growing, although robotic-assisted CRS/HIPEC remains rare in routine clinical practice.
Conclusion
Robotic-assisted CRS/HIPEC can be safe in carefully selected patients and accelerate postoperative recovery.
Case presentation
A 37-year-old patient was referred to gynecology for further investigation of an ovarian cyst. During resection, the large cyst originating from the left ovary ruptured. Histological analysis revealed a mucinous epithelial tumor with immunohistochemical intestinal differentiation of unknown origin. Further investigations (PET-CT, gastroscopy, colonoscopy, appendectomy) found a LAMN, pT4a, R0 with PCI 5. Following multidisciplinary tumor board discussion (MDT), we performed a robotic-assisted CRS/HIPEC as follows using the da Vinci Xi® (video sequences):
(1) Incisions: horizontal line at the umbilicus (for double docking technique)
(2) Diagnostic laparoscopy: PCI 8
(3) Mobilization of liver, stripping of liver capsule, splenectomy
(4) Peritonectomy of right upper quadrant and diaphragm
(5) Peritonectomy of left diaphragm, omentectomy,
(6) Redocking of da Vinci, targeting for lower abdomen
(7) Bilateral adnexectomy
(8) Rectal-sparing pelvic peritonectomy
(9) Specimen retrieval via Pfannenstiel incision, CCR-0
(10) Placing of tubes, HIPEC: Mitomycin C (35 mg/m²), 41–43 °C, 90 minutes
(11) Abdominal rinsing (saline) and closing of incisions
Uneventful postoperative course with discharge on day 6 after surgery. Histology confirmed acellular mucin deposits across all resected peritoneal surfaces, splenic involvement, and infiltration of both ovaries. Postoperative MDT recommended regular abdominal imaging for follow-up.
Clinical Benefits and Economic Challenges of Large-Scale Postoperative Telemonitoring: A University Hospital Experience
Abstract
Background
Digital health solutions enable patient support during the critical postoperative period through direct communication with the provider and standardized symptom surveillance, facilitating early detection of complications and reducing in-person visits and readmissions. Following a colorectal surgery pilot study, the follow-up program was scaled institution-wide with a 24/7 monitoring centre.
Aims
To assess clinical outcomes, patient compliance and satisfaction, and to provide a cost-revenue analysis of the telemonitoring strategy.
Methods
A retrospective study in a tertiary referral centre. Data were extracted from electronic patient records and the telemonitoring platform for patients followed between May 1, 2021, and April 30, 2024. Cost and reimbursement data were obtained from the hospital’s cost accounting and coding systems. The cost-revenue analysis was performed using a micro-costing approach, including direct medical costs and reimbursement.
Results
2876 patients were telemonitored, including 378 visceral surgery patients. Overall, 1926 (67%) patients generated at least one alert, most related to pain (46.1%), wound complications (13.2%), and respiratory symptoms (12.9%). Among visceral surgery patients, 80% generated alerts, most related to bowel function (30.6%), wound complications (30.6%) and pain (19%), almost exclusively managed remotely. The 30-day overall complication rate was 13.5%, occurring on average on postoperative day 7 ± 6. Nearly half of complications arose after discharge, with half of these detected through telemonitoring. Overall, 95% of patients reported being satisfied with the telemonitoring solution. An estimated 424 medical visits were avoided, saving CHF 166,100 in direct costs. For visceral surgery patients, the hospital incurred a deficit of CHF 440,760, partly due to low-outlier reimbursement cuts.
Conclusion
Large-scale postoperative telemonitoring is feasible, safely detects early post-discharge complications, reducing unplanned in-person visits, and generates high patient satisfaction. Although it may reduce costs at the healthcare system level and support outpatient strategies, it can generate financial losses for hospitals, potentially discouraging the adoption of valuable digital health solutions.
HPB II
Transition from an open to a robotic liver surgery program
Abstract
Background
The adoption of robotic liver surgery (RLS) represents a major innovation in hepatobiliary surgery, with improved perioperative outcomes. Compared to open liver surgery (OLS), RLS offers several advantages. We compared a two-year OLS phase (phase 1) with the follwing two-year RLS implementation phase (phase 2) focusing on case selection and surgical outcomes.
Aims
The aim of this study was to describe the institutional transition from a pure OLS program to a RLS program in a center without previous experience in laparoscopic liver surgery.
Methods
This retrospective, single-center cohort study was conducted at a tertiary referral center for hepatobiliary surgery with an annual case-load of around 100-110 liver resections. All consecutive patients undergoing liver resection between 01/2020 and 06/2025 were included, RLS started in 01/2023. Inclusion criteria comprised adult patients undergoing any form of liver surgery for benign or malignant indications.
Results
A total of 445 patients were included, of whom 346 (78%) underwent OLS and 99 (22%) RLS. Major resections were performed in 47% of OLS and 20% of RLS. After RLS implementation 45% of all cases were performend robotically. Compared to phase 1, major complications dropped from 40% to 21% (p<0.001). Both post-hepatectomy liver failure (PHLF) (6% vs. 4%; p=0.403) and bile leak were comparable (8% vs. 9%; p=0.119) in the two phases. Length of stay (LOS) was reduced from 11 (8-16.5) to 7 (5-10) days.
Comparing the overall cohort of OLS with RLS, major complications (OLS : 38% vs RLS: 7%), PHLF (OLS : 6% vs RLS: 0%), and biliary leakage (OLS : 9% vs RLS: 3%), ocurred more often after OLS. Similarly, LOS was reduced for RLS compared to OLS (5 (4-7) vs. 10 (7-15) days).
Conclusion
Even without prior laparoscopic experience, a structured transition to robotic liver surgery allows a minimally invasive appraoch in every other patient. The transition to robotic liver surgery is associated with substantially reduced morbidity and shorter hospitalization.
One-hundred consecutive robotic liver resections: initial experience and lessons learned
Abstract
Background
Following prior open and laparoscopic experience, robotic liver resection (RLR) was introduced in early 2023.
Aims
To analyze the results of the first 100 RLRs.
Methods
Data of consecutive RLRs (02/2023 to 11/2025) were prospectively collected. The primary endpoint was postoperative morbidity; secondary ones included other clinical outcomes within 90-days after surgery. Subgroup analysis included patients with repeat hepatectomy, multiple resection areas, RLRs complexity based on the Iwate criteria. Kruskal-Wallis and Chi-square tests were used for subgroup comparisons.
Results
In 100 consecutive patients (40% females, mean age 65 years, mean Charlson-comorbidity-index 7), main indications were hepatocellular carcinoma (n=38), colorectal-liver-metastases (n=32). Cirrhosis rate was 28%, and 18% of patients underwent repeat hepatectomy (prior hepatectomy≥1). Mean number of nodules was 2.2, involving posterior-superior liver segments in 54%. Non-anatomic resections were performed in 54%, and multiple resection areas in 32% of cases (range 2-9) with mean blood loss of 200 cc. Non-urgent conversion to laparotomy occurred in 4% and intraoperative ablation was associated with RLR in 13% of cases. Postoperative overall and major morbidity (CD≥3) rates were 26% and 7% respectively (grade B post-hepatectomy liver failure 2%, biliary leak 1%), without reoperations. Overall morbidity was nihil after repeat hepatectomies and similar in patients with one (25%) vs. multiple resections (28%). Mean hospital stay was 6 days, with 90d readmission of 6%. Mortality was 1% (massive myocardial infarction). Textbook outcomes were reached in 79% of RLRs. Based on Iwate criteria RLR difficulty was low (n=25), intermediate (n=46), advanced (n=21) or expert (n=8). Operative time, blood loss, hospital stay increased with increasing difficulty, while complications and textbook outcomes remained stable.
Conclusion
Transition to robotic hepatectomy could be safely achieved, with good short-term results maintained in complex subgroups like repeat hepatectomies, multiples resections or high Iwate scores.
Major Liver Resection in Cirrhotic HCC patients in the era of robotic surgery: Expanding Boundaries of Surgical Therapy
Abstract
Background
Cirrhosis has traditionally been considered a relative contraindication for hepatic resection due to the risk of post-hepatectomy liver failure (PHLF). With the rising incidence of HCC and persistent organ shortage, alternative curative approaches are urgently required. Robotic surgery may provide improved outcomes, less invasiveness, and be particularly beneficial for cirrhotic patients.
Aims
To evaluate the safety and outcomes of robotic liver resection in cirrhotic HCC patients.
Methods
We retrospectively analyzed all cirrhotic patients with HCC undergoing liver resection between 2020–2025. Patients were stratified by approach (open, laparoscopic, robotic).
Results
Fifty-seven (n=57) cirrhotic patients underwent liver resection for HCC: open (n=28), laparoscopic (n=7), and robotic (n=21). Whereas initially major resections accounted only for 17% (n=6/35) of open and laparoscopic resections, the initiation of the robotic program significantly increased the rate of major resections up to 43% (n=9/21). Despite a learning curve, overall median operative time was comparable between open and robotic resections (242 vs. 252 minutes, p=0.64), whereas robotic procedures significantly reduced operation time compared with equivalent laparoscopic resections from 214 to 198 minutes (p=0.03). With proportional increase of major liver resections, a trend to bigger tumor size and frameshift from BCLC 0 to BCLC A patients was observed for the robotic group. In that context, PHLF occurred in n=3/6 robotic major resections (all ISGLS grade A, resolved with supportive care) versus n=2/9 severe grade C cases after open surgery. Despite more complex resections, robotic patients had shorter ICU stay (1 vs. 3 days, p=0.01) and reduced hospital stay (7 vs. 11 days, p=0.02). No conversion and no mortality occured for robotic resections. R0 rates were comparable (98% vs. 96%, p=0.89).
Conclusion
Robotic hepatectomies are safe in selected cirrhotic HCC patients. Although mild PHLF was common, recovery outcomes are favorable. Therfore, in the era of organ shortage, robotic surgery can expand resectional options.
Clinical Practice of Indocyanine Green Fluorescence Imaging in Robotic Liver Surgery – a Global Expert Survey
Abstract
Background
Indocyanine green (ICG) fluorescence imaging is increasingly incorporated into robotic liver resections (RLR), yet clinical practice regarding timing, dosage, and staining techniques is divergent.
Aims
This international expert survey aimed to characterize current practices for ICG in RLR.
Methods
Experts in RLR were invited to participate based on surgical volume (experience of 50 RLR and 30 annual RLR). A 74-item questionnaire was developed following a literature search and reviewed by a steering committee. The survey addressed indications, timing, dosage, imaging technology, benefits, limitations, training, and future directions of ICG use. Responses collected between September and October 2025 were analyzed.
Results
Seventy experts from 19 countries completed the survey, corresponding to an 88% response rate. Centers performed a median of 180 annual liver resections, including 55 RLR. Most experts used ICG (96%) during RLR. Anatomical demarcation (91%), tumor localization (60%), and biliary anatomy assessment (60%) were the most frequent indications. 60% of experts use preoperative ICG, while intraoperative ICG is mainly administered for demarcation (67%) and biliary tract visualization (40%). Considerable heterogeneity exists in dosage, timing, and staining techniques, particularly in cirrhotic livers and for tumor localization. Only half of the experts had standard operating procedures, whereas 64% expressed the need for a higher degree of standardization. Reported benefits of ICG use included improved anatomical orientation, margin assessment, lesion detection, and support during complex resections. Perceived limitations included background fluorescence, tissue penetration and variable staining in diseased parenchyma. 80% anticipated improved outcomes with combined ICG and three-dimensional image-guidance.
Conclusion
ICG fluorescence is widely used in RLR and is an important cornerstone for precision-guided robotic liver surgery. Standardized clinical practice guidelines, structured training, and technological improvements in imaging and navigation systems are claimed to optimize its clinical use.
Economic Impact of Robotic Liver Resection - A Systematic Review of Costs, Resource Utilization, and Length of Stay
Abstract
Background
Robotic liver resection (RLR) is increasingly adopted in hepatobiliary surgery due to perioperative advantages. However, its economic impact remains controversial, particularly in comparison with open liver resection (OLR) and laparoscopic liver resection (LLR).
Aims
This systematic review aimed to evaluate the existing evidence on costs, resource utilization, and length of stay associated with RLR in adult liver surgery.
Methods
A systematic review was conducted in accordance with PRISMA and AMSTAR-2 guidelines and registered with PROSPERO. MEDLINE, EMBASE, and the Cochrane Library were searched up to September 2025. Studies reporting cost analyses of RLR for benign or malignant liver disease were included. Primary outcomes were total hospital costs and length of stay (LOS). Secondary outcomes included intraoperative, postoperative, readmission, and indirect costs. Study quality was assessed using the Drummond checklist.
Results
Thirty-two observational studies comprising 17,016 patients were included. RLR was consistently associated with higher intraoperative costs compared with OLR and LLR, largely driven by consumables and robotic instrumentation. Despite this, most studies comparing RLR with OLR reported comparable or lower total costs for RLR, primarily due to reduced LOS, fewer complications, and lower readmission rates. Median postoperative LOS was shorter with RLR than OLR in nearly all studies. Comparisons between RLR and LLR showed more heterogeneous results, with laparoscopy generally associated with lower total costs, although selected high-volume centers reported cost equivalence or lower costs with RLR. Only 25% of studies incorporated indirect costs such as robotic platform acquisition and maintenance. Overall study quality was predominantly rated as average.
Conclusion
RLR incurs higher intraoperative costs but may achieve comparable or reduced total hospital costs relative to open surgery through reduced LOS and complication burden. Compared with laparoscopy, a consistent economic advantage for RLR is less evident and appears context dependent. Future high-quality economic evaluations incorporating indirect costs and standardized cost definitions are required to better define the cost-effectiveness of RLR within modern hepatobiliary practice.

Mutli-center Analysis of Surgical Outcomes after Simultaneous Robotic Resection of Primary Colorectal Cancer and Liver Metastasis
Abstract
Background
Colorectal cancer (CRC) is the third most common cancer and the second leading cause of cancer death worldwide. The liver is the most common site of metastatic disease, with an estimated 15-20% of patients presenting with synchronous colorectal liver metastasis (LM). While overall robotic resections are increasingly performed due to the beneficial effects for patients and surgeons, scientific data on outcomes of simultaneous robotic (CRC and LM) resections is scarce.
Aims
The aim of this observational study is to analyze outcomes after simultaneous robotic resections of primary CRC and LM.
Methods
This oberservational multi-center cohort study analyzed 23 patients undergoing simultaneous robotic hepatic and colorectal resection for metastatic CRC at 3 tertiary care centers. All patients were ≥18 years and underwent surgery from 01/2018 to 07/2025.
Results
Twenty-three patients underwent simultaneous robotic resection of CRC and LM at 3 centers. Median hospital stay was 4 days (mean 5.61, SD 2.95). The highest Clavien–Dindo complication grade was IIIa in 1 patient (4.35%) during index admission and at 90 days. The 90-day Comprehensive Complication Index showed a median of 0 (mean 9.50, SD 12.86). No colonic anastomotic leaks or postoperative hemorrhage occurred. Biliary leakage was observed in 4 patients (17.39%; Grade A n=3, Grade B n=1, Grade C n=0). Postoperative liver failure occurred in 2 patients (8.70%; Grade A n=1, Grade C n=1). R0 resection was achieved in all colonic specimens (100%) and in 21 hepatic specimens (91.30%). Thirty-day mortality was 0%.
Conclusion
Simultaneous robotic resection of primary CRC and synchronous LM appears to be a safe and feasible surgical strategy when performed in experienced centers. Favorable short-term perioperative outcomes with preserved oncologic quality are demonstrated. The findings support further adoption of the robotic approach and warrant larger prospective studies to confirm long-term oncologic benefits and define optimal patient selection.
Postoperative Alpha-Fetoprotein as a Predictive Marker in Patients With Hepatocellular Carcinoma After Liver Resection
Abstract
Background
Recurrence after curative-intent hepatic resection for hepatocellular carcinoma (HCC) remains prominent. Alpha-fetoprotein (AFP) is used for prognostic assessment, with most studies relying on dichotomised cut-offs. The prognostic value of early postoperative continuous AFP remains insufficiently assessed.
Aims
To evaluate the association of AFP at three months after resection for recurrence-free survival (RFS).
Methods
Single centre, retrospective study of adult patients undergoing curative-intent hepatic resection for HCC, with AFP measurements at 3 months. Patients with recurrence prior to laboratory assessment were excluded. RFS was assessed using a 3-month landmark Cox proportional hazards regression model. Smoothed hazard regression using restricted cubic splines was performed. Multivariable Cox regression adjusted for tumour size and multifocality. Discriminatory performance was assessed using a 1-year time-dependent area under the receiver operating characteristic (AUROC).
Results
Among 320 eligible patients, AFP values were available in 201 (62.8%) preoperatively and 94 (29.4%) at 3 months, 103 (32.2%) at 6 months, and 113 (35.3%) at 1-year. After exclusion of early recurrence (n=17) and patients with missing data on either tumour size or multifocality (n=4), 73 patients were analysed. Median AFP at 3 months was 3.6mg/L (IQR:2.5-7.4), and 46 (63.0%) had AFP <5mg/L. During median follow-up of 6.7 years from the 3-month landmark (IQR:2.8-8.9), 46 (63.0%) developed recurrence. Landmark RFS at 1-, 3-, and 5-years was 59.0%, 35.9% and 25.8%, median RFS of 1.6 years (IQR:0.4-7.1). Higher AFP levels at 3 months were strongly associated with recurrence (HR 1.35 per unit increase in log-transformed AFP, 95% CI:1.11-1.62; p=0.008) (Figure 1). No evidence of non-linearity between AFP and recurrence risk was observed (p=0.40). After adjustment for tumour size and multifocality, AFP remained independently associated with recurrence. The 1-year time-dependent AUROC was 0.58.
Conclusion
AFP after hepatic resection is independently associated with recurrence risk when analysed as a continuous variable but demonstrates only moderate discriminatory performance.
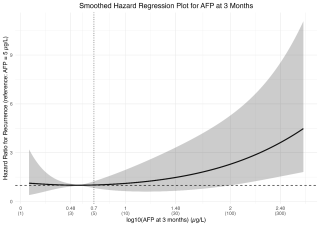
Thoracic Surgery - Free Communication 2
Joining Forces - Bridging Science and Surgery
Endothelial-to-Mesenchymal Transition in Fibrotic Lesion Formation in CTEPH
Abstract
Background
Chronic thromboembolic pulmonary hypertension (CTEPH) is a rare, progressive form of pulmonary hypertension caused by persistent obstruction of the pulmonary arteries (PAs) following unresolved pulmonary embolism (PE). Only a subset of PE patients develop CTEPH, suggesting underlying endothelial vulnerability. We hypothesize that pulmonary artery endothelial cell (PAEC) dysfunction contributes to CTEPH pathogenesis by promoting vascular remodeling and fibrosis through endothelial-to-mesenchymal transition (EndMT).
Aims
Determine how endothelial dysfunction predisposes pulmonary artery endothelial cells to EndMT in CTEPH compared with control pulmonary arteries
Methods
Intimal and fibrotic tissues obtained from pulmonary endarterectomy (PEA) specimens and pulmonary artery tissue collected during lung transplantation (LTP) in 2025 were used to isolate PAECs. Cell proliferation and barrier function were assessed using the MTT assay and electric cell–substrate impedance sensing (ECIS) technology, respectively. To evaluate the potential for EndMT, PAECs were exposed to an artificial clot generated by thrombin-induced plasma coagulation, mimicking the post-embolic environment.
Results
We established a robust protocol for culturing PAECs from intimal material removed during PEA in CTEPH patients and from pulmonary artery tissue obtained during LTP as controls. Endothelial identity was confirmed by cobblestone morphology, positive staining for CD31 (PECAM-1) and von Willebrand factor (vWF), and absence of α-smooth muscle actin (α-SMA), excluding contamination by myofibroblasts. Functional assays demonstrated that CTEPH-derived PAECs exhibit hyperproliferation and reduced barrier integrity compared to control cells. Upon exposure to the artificial clot, CTEPH PAECs showed morphological changes consistent with EndMT and impaired clot degradation, suggesting altered endothelial function and matrix interaction.
Conclusion
Our findings demonstrate, for the first time, that CTEPH PAECs are predisposed to EndMT and impaired thrombus resolution, potentially driving vascular remodeling. Ongoing work will employ bulk and spatial transcriptomics to define molecular pathways and cell–cell interactions underlying endothelial plasticity in CTEPH.
Exosomal RNA Profiling Identifies Long Noncoding RNAs and Protein Coding Genes as Potential Circulating Diagnostic Biomarkers for Pleural Mesothelioma
Abstract
Background
RNAs secreted by tumor cells via exosomes that are detectable in biological fluid such as plasma, have emerged as promising biomarkers for non-invasive cancer diagnosis.
Aims
This study aimed to compare the RNA cargo of exosomes secreted by primary Pleural Mesothelioma (PM) cells with those from non-PM cells, to identify circulating biomarkers that potentially could be used as non-invasive diagnostic biomarkers for PM.
Methods
Primary cell cultures were established from pleural effusions of 12 PM and 7 non-PM patients. Exosomes were isolated from cell culture supernatants using iZON qEV columns, followed by total RNA extraction using the mirVana PARIS kit and RNA sequencing. Sequencing reads were mapped to the human reference genome (GRCh38), and differential expression analysis was performed using DESeq2 to identify RNAs enriched in PM-derived exosomes. Candidate RNAs were validated in exosomes from cell cultures using RT-qPCR.
Results
We identified 2,089 RNAs upregulated in PM-derived exosomes with the majority comprising long noncoding RNAs (lncRNAs) (34%), pseudogenes (30%), and protein-coding genes (27%). Among the lncRNAs, GAS5 - a gene that we previously characterized functionally in PM - emerged as a particularly promising candidate for PM diagnosis. RT-qPCR validation of cell culture exosomes confirmed significantly higher GAS5 expression in exosomes from PM compared to non-PM samples. Next, we performed a one‑step multiplex probe assay using digital PCR to simultaneously detect three gene targets and two loading controls in clinical samples from three patients. We successfully identified two candidate genes (CACYBP and RSL1D1) in total plasma. We detected one candidate gene, CACYBP, in pleural effusion-derived exosomes, interestingly, at higher levels compared to matched plasma samples. Notably, the levels of all the five genes remained below the detection limit in plasma-derived exosomes.
Conclusion
Our findings emphasize the potential utility of the PM exosomes for PM detection and highlight GAS5, CACYBP and RSL1D1 as potential diagnostic biomarker candidates. Further large-scale analysis is needed to establish their clinical utility.
Minimally invasive porcine in vivo model for chronic thromboembolic pulmonary hypertension
Abstract
Background
Chronic thromboembolic pulmonary hypertension (CTEPH) is often associated with preceding pulmonary embolisms developing bilateral fibrotic obstructions of the pulmonary arteries (PA) and microvascular changes. To understand the complex underlying pathophysiology, research relies on in vivo models. A large animal model has been developed to mimic characteristics of CTEPH using invasive techniques such as ligation of the PA via sternotomy.
Aims
Considering animal welfare and 3R principles, we aim to refine and develop a minimally invasive CTEPH model.
Methods
We studied five female large white pigs (50kg, 3-4 months). Under general anesthesia and hemodynamic monitoring, an intravascular plug was inserted into the left PA. The right lower lobe artery was embolized with non-resolving n-butyl-2-cyanoacrylate glue. Glue-embolization was repeated weekly for 5 weeks. MRI assessment was performed at each intervention. At week 5 macro- and microscopic lung assessment and plasma molecular analysis were performed.
Results
Implantation of the intravascular plug in the left PA was successful in all animals, without any residual perfusion seen in MRI angiography. The mPAP increased from 15.6mmHg (SD 3.5) at baseline to 35mmHg (SD 7.7) (p = 0.005) at week 5. Functional cardiovascular MRI showed an increase in right ventricle dimension. Macroscopically, the left lung showed areas of ischemia with hypertrophy of bronchial arteries and overperfusion in the right upper lobe. Histologically, microvascular wall thickness was increased in both the hyperperfused (right upper lobe) and ischemic territory (left lung). Plasma molecular analysis revealed elevated circulating endothelin-1 and reduced nitric oxide metabolites associated with CTEPH development.
Conclusion
We established a minimally invasive approach for a previously described CTEPH model, including representative hemodynamic, morphological and molecular CTEPH features. The model increases safety and welfare for experimental animals.
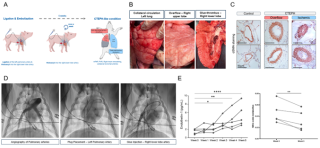
Hyperthermic Intrathoracic Cisplatin Promotes Immunogenic Cell Death in Malignant Pleural Mesothelioma
Abstract
Background
Malignant pleural mesothelioma (MPM) remains a major therapeutic challenge, with conventional treatments providing limited benefit. Prior studies in patients with MPM have shown that hyperthermic intrathoracic chemotherapy (HITOC) could improve patient survival. Recently, in a preclinical murine model of MPM, we demonstrated that HITOC enhanced intratumoral CD8⁺ T-cell infiltration and synergized with dual PD-1/CTLA-4 blockade improving cancer control. However, the initial mechanisms induced by HITOC causing microenvironment immunomodulation remain unclear.
Aims
In this study, we examined the potential of HITOC to induce immunogenic cell death (ICD) in MPM, promoting the release of damage-associated molecular patterns (DAMPs) and subsequent immune activation.
Methods
AB12 MPM cells were exposed to vehicle or cisplatin (100 μM) under normothermic (37 °C) or hyperthermic (40 °C) conditions for 60 minutes to mimic intraoperative HITOC conditions. At several time points after treatment, multiple measurements were made including: (1) monitoring of cell viability using MTS and lactate dehydrogenase (LDH) assays; (2) quantification of global proteomic changes by liquid chromatography–tandem mass spectrometry; (3) evaluation of ICD-associated DAMPs HSP70, HSP90 and ATP by immunofluorescence, western blotting and bioluminescence
Results
AB12 cell viability was reduced by normothermic and further reduced by hyperthermic cisplatin at 24 hours (n=6). Proteomic profiling at 24 hours revealed marked alterations in cisplatin-treated cells but not in response to hyperthermia (n=3). At early timepoints however, heat adjunct to cisplatin increased HSP70 and HSP90 expression 6 hours post-treatment, with HSP90 upregulation sustained up to 24 hours compared to normothermic cisplatin. Hyperthermic cisplatin caused increased levels of extracellular ATP (peak at 12 hours, n=3) which returned to baseline levels at 24 hours, consistent with early DAMPs release characteristic of ICD.
Conclusion
Hyperthermic cisplatin induces tumor cell death with immunogenic features in MPM cells. These results provide the initial mechanistic steps of HITOC-induced immune activation. Further studies are required to confirm these data in vivo.
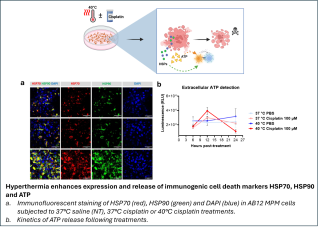
Clonal Evolution and Intratumoral Heterogeneity in Metachronous Oligometastatic Non-Small Cell Lung Cancer: The Role of Surgery for Multiregional Tissue Analysis
Abstract
Background
In oligometastatic non-small cell lung cancer (NSCLC), the combination of systemic therapy and local ablative treatment (LAT) including surgery and radiotherapy has been shown to provide a substantial survival improvement. However, patient selection for LAT remains a central challenge – mostly because the biology and molecular characteristics of “true” oligometastatic disease (OMD) is still poorly understood.
Aims
Here we aimed to perform a comprehensive next-generation sequencing (NGS) of sequentially resected tissue specimens from metachronous OMD.
Methods
Patients with metachronous oligorecurrent NSCLC (≤5 metastases in ≤3 organs) and representative sequential tissue specimens were identified from a prospectively maintained RedCap Database. Primary tumor resection was performed between 01/2016 and 12/2024 at a single institution. NGS was performed using the Oncomine Comprehensive Assay Plus. Clonal hierarchies were reconstructed for each tumor based on variant allele frequencies (VAF) of somatic alterations.
Results
NGS was successfully performed on 19 cancer specimens (primary tumors and metastases) from 6 patients. Adenocarcinoma was present in five patients and squamous-cell carcinoma in one patient. Initial UICC stages were IA3 (n=1), IIIA (n=3) and IVB (OMD; n=2). Oligorecurrence occurred after a median (IQR) of 16.5 (9.2-47.6) months. Analysis of clonal hierarchy revealed KRAS, TP53, EGFR, and NRAS as truncal mutations in three, two, one and one patients, respectively. Subclonal somatic changes were common and included low-level genetic alterations in known therapy relevant genes such as STK11 and KEAP1.
Among three patients with consecutive brain metastases, genetic profiles of the resected tissue specimens showed a high clonality in evolution with maintained mutational profiles in all paired specimens. Conversely, extracranial metastases demonstrated a more divergent evolution where only the truncal mutations were maintained in metastases.
Conclusion
Surgical resection of primary tumors and distant metastases not only offers LAT, but also allows a multiregional tissue analysis to understand clonal evolution in OMD. Subclonal alterations may eventually occur but the complexity of clonal evolution appears to be highly variable among patients with OMD.

"One-Stop Shop" From Diagnosis to Resection for Suspicious Pulmonary Lesions: Early Outcomes From a Stage-Matched Comparative Study
Abstract
Background
Since the first implementation of a CT-guided robotic navigation bronchoscopy program in Europe in our centre in July 2024, we have established a One-Stop Shop (OSS) concept for patients with suspicious pulmonary nodules, consisting of: Robotic-assisted navigation-bronchoscopy (ION) with integrated cone-beam CT, biopsy, marking of the nodule with fiducial and ICG, fresh-frozen examination and direct oncological resection in one general anaesthesia.
Aims
The idea behind the concept was to shorten patient pathways and reduce psychological burden during waiting times, which is proven to affect overall survival in NSCLC patients (1, 2).
Methods
Comparison of the first 37 patients undergoing our OSS concept to UICC-stage-matched (1:1) control group (n=37), in which patients had preoperative transbronchial biopsy or wedge-resection for diagnostic purposes. Time period was compared from first CT-scan with suspicious lesion to treatment.
Results
There was no relevant difference regarding median age (69.5 vs. 70 years; p=0.955) and gender (p=0.67) between the two groups. 43.2% percent of the patients had an UICC-Stage IA1, 32.4% IA2, 8.1% a pulmonary metastasis and 8.1% a benign finding (Figure 1A). In both groups, all surgeries were performed by a minimal-invasive approach (VATS/RATS). Time from first CT-scan with suspicious lesion to treatment was shorter in the OSS cohort (45 days vs. 58 days respectively, p=0.032). In a subgroup analysis of NSCLC patients, this effect was even more pronounced compared to the control group (45 days vs. 65 days, p=0.025) (Figure 1B). There was no difference in hospitalisation after resection between the groups (median 3 days for both, p=0.81) (Figure 1C).
Conclusion
Our OSS approach enables rapid diagnosis and treatment of potentially malignant pulmonary lesions in patients eligible for primary resection, minimizing delays in care. Furthermore, the OSS has the potential to reduce psychological stress in patients, which can positively impact survival rates. In this regard, an RCT is currently planned.
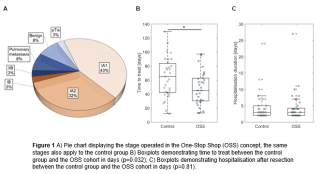

Pushing the Limits of Robotic-Assisted Thoracic Surgery: Outcomes of Anatomical Lung Resection After Neoadjuvant Immune Checkpoint Inhibitor Treatment for Advanced Non-Small Cell Lung Cancer
Abstract
Background
Induction treatment with immune checkpoint inhibitors (ICI) improves survival and pathological response in locally advanced and oligometastatic non-small cell lung cancer (NSCLC). However, neoadjuvant ICI treatment may increase surgical complexity due to hilar fibrosis and higher conversion rates have been reported.
Aims
We therefore aimed to assess perioperative outcomes of robotic-assisted thoracic surgery (RATS) after neoadjuvant immunotherapy or chemo-immunotherapy.
Methods
From a prospectively maintained database, we identified patients with histologically confirmed UICC stage II-IV NSCLC who were treated with ICI or chemo-ICI prior to RATS anatomical lung resection between June 2019 and August 2025. Patients included in ongoing clinical trials were excluded. Surgical complexity was assessed by review of operative reports according to the proposed scoring system by Rusch et al. (JTCVS 2023).
Results
24 patients who received RATS anatomical lung resection were analyzed, including 8 stage IIB, 8 stage IIIA, 1 stage IIIB, 5 stage IVA and 2 stage IVB patients. Resections included 22 lobectomies, 1 segmentectomy and 1 extended pneumonectomy. The overall conversion rate to thoracotomy was 12.5% (3 out of 24 patients), due to extensive hilar fibrosis. R0-resection was achieved in all patients. Postoperative complications included pneumothorax requiring chest tube placement (Clavien-Dindo grade 3) in 3 patients. No postoperative complications of grade 4 or higher occured. Higher surgical complexity was associated with increased operative time, although not statistically significant (p=0.063). Increased surgical complexity did not affect the length of hospital stay (p=0.77). Nodal downstaging to pN0 was seen in 83.3% of patients with cN1 disease (n=5/6), 71.4% of patients with cN2 disease (n=5/7) and 100% of patients with cN3 disease (n=2/2).
Conclusion
In this single-center cohort, the RATS approach enables a safe anatomical resection of locally advanced and oligometastatic NSCLC after ICI treatment with low conversion rates despite high surgical complexity. Postoperative complications were low-grade and well manageable.
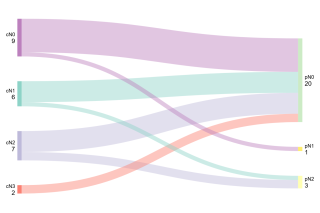
Intraoperative CT Imaging for Real-Time Nodule Visualisation and Margin Measurement in Sublobar Lung Resection: A Retrospective Study
Abstract
Background
Achieving negative resection margins in non-small cell lung cancer (NSCLC) is essential, as is ensuring accurate excision of the target nodule and avoiding incomplete or misplaced resections. Intraoperative computed tomography (iCT) may confirm nodule visualisation and support real-time margin assessment at the staple line.
Aims
To assess the feasibility of specimen-based iCT for nodule visualisation and compare iCT-derived margins with pathology-confirmed margins, as well as radiologist-reported findings on iCT versus pre-operative CT.
Methods
We retrospectively included consecutive adult patients undergoing therapeutic sublobar resection for suspected or confirmed NSCLC with ex vivo specimen iCT performed intraoperatively using a mobile cone-beam CT system. Nodule visualisation on iCT was classified as good, uncertain, or not visualised based on the radiology report. The iCT margin was the minimal distance from the nodule to the staple line; the reference standard was histopathology. Continuous measurements were compared using Bland–Altman agreement analysis and categorical variables using kappa.
Results
Thirty-two patients were analysed (median age 68 years; 16 females); The preoperative indication for resection was a suspected malignant pulmonary nodule in 27/32 (84.4%) patients and confirmed NSCLC in 5/32 (15.6%) (prior history or biopsy-proven). Nodules were visualised on iCT in 30/32 (93.8%) and classified as uncertain in 2/32 (6.2%). R0 was achieved in 32/32 (100%). For the largest solid component (29 paired measurements), the nodules appeared larger in pre-operative CT than iCT with a mean bias of +0.79 mm (limits −8.84 to +10.43 mm); pathology measurements were larger than imaging (bias −4.19 mm vs pre-operative CT; −4.76 mm vs iCT). For staple-to-tumour margins, iCT versus pathology showed mean bias −1.08 mm (limits −19.27 to +17.10 mm).
Conclusion
Portable iCT is feasible for intraoperative nodule visualisation, helping to avoid incomplete or misplaced resections. Agreement with pathology for staple-to-tumour distance showed substantial variability, supporting iCT as an adjunct rather than a substitute for histopathology.
Coffee Break
Go beyond laparoscopy, stay MIS, take the curve with articulated sealing
Sharing expertise with experts
Expert exchange in a relaxed atmosphere at the B. Braun Medical booth
Tutor: Ian Fournier, Sion
Bridging the Gap. Do We Still Need to Teach Robotic Natives in Laparoscopy?

Clinical Learning – the Robotic Learning Curve
Safety Curriculum – the Industry Perspective
The Psychology of Learning – How Video Gaming Affects Learning
Panel Discussion
The Chair's View
The Industry's Perspective
The Resident's View
The UK Perspective
The Swiss College of Surgeon's View
Challenging Cases: Case-Based Discussion
My Most Challenging Aorto-iliac Case
My Most Challenging Lower Extremity Case
My Most Challenging Aortic Aneurysm Case
EPAs
A Must-Have
An Administrative Burden
Where Are We Heading: Vision With EPAs
An Example of How it Works
Reality Check From a Resident
Hernia
Prophylactic mesh augmentation in midline laparotomy in elective or emergency settings: A systematic review and network meta-analysis of randomized trials
Abstract
Background
Incisional hernia (IH) after midline laparotomy occurs in 5-20% of patients, and can reach 30% in high-risk settings. Cost for IH repair was estimated at $15,899 per case in 2006. Although current guidelines support prophylactic mesh augmentation, the optimal anatomical plane, particularly in emergency settings, remains controversial. We conducted a systematic review and a network meta-analysis (NMA) of randomized trials (RCT) to compare mesh positions for IH prevention.
Aims
To identify the optimal prophylactic mesh plane for preventing IH after midline laparotomy in elective or emergency settings.
Methods
A systematic search of Pubmed, Embase and Cochrane databases was performed, including RCT on prophylactic mesh augmentation after midline laparotomy. Primary outcome was IH incidence. Secondary outcomes were surgical site occurrence (SSO), and surgical site infection (SSI). Elective and emergency settings were included. A random-effect NMA with Bayesian comparison was performed.
Results
27 RCT, including 4298 patients, were analyzed (20 elective, 7 emergency). Control group was suture-only closure (1891 patients). Mesh positions were onlay (OM, 38%), retromuscular/preperitoneal (RM/PP, 37%), intraperitoneal (IP, 19%), and inlay (IM, 7%). Overall, mesh augmentation significantly reduced IH incidence (RR 0.41, 95% CI 0.27-0.62). Our analysis showed that both OM and RM/PP are the most effective techniques. OM ranked highest for IH prevention in both elective (RR 0.19, 95% CI 0.07-0.40), and emergency settings (RR 0.22, 95% CI 0.02-0.98), whereas RM/PP was not statistically significant in emergency surgery. Mesh augmentation increased SSO risk (RR 1.38, 95% CI 1.06-1.79), particularly with OM (RR 1.59, 95% CI 1.03-2.55). SSI rates were not significantly increased, irrespective of mesh positions or surgical settings.
Conclusion
Prophylactic mesh augmentation effectively reduces IH after midline laparotomy. OM provides the best prevention of IH, including in emergency surgeries, at the cost of increased SSO. These findings support OM or RM/PP as valid preventive strategies, with individualized risk-benefit assessment.
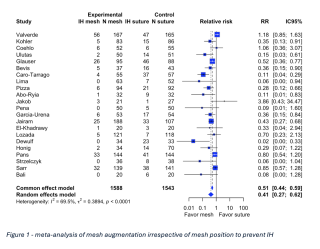
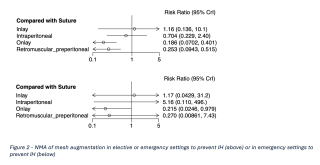
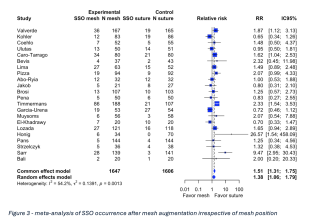
Robotic Minimally Invasive Ventral Hernia Repair With the DEXTER Robotic Surgery System (RAVEN)
Abstract
Background
In ventral and incisional hernia repair, robotic approaches have expanded the surgical armamentarium, particularly for extraperitoneal and retromuscular reconstructions, offering improved ergonomics, enhanced visualization, and facilitation of intracorporeal suturing. After perioperative safety and feasibility of the DEXTER Robotic Surgery System have been demonstrated in inguinal hernia repair and cholecystectomy, its application in ventral hernia repair remains to be evaluated.
Aims
The aim of this clinical study was to confirm the perioperative and early postoperative safety and clinical performance of the DEXTER Robotic Surgery System in patients undergoing incisional or primary ventral hernia repair.
Methods
We conducted a prospective study at five centers in France, Germany, and Switzerland (ClinicalTrials.gov Identifier NCT07071740) including seven surgeons. Eligible patients presented with incisional or primary midline ventral hernia smaller or equal to 8 cm. The primary objectives of the study were to document the successful completion of the ventral hernia repair procedures and to collect data on the occurrence of major complications (Clavien-Dindo grades III-V), and other adverse events perioperatively and up to 30 days post-surgery.
Results
33 patients were operated for ventral hernia repair with eTEP (2), IPOM+ (2), TARUP (9) and TAPP (20) techniques. The mean age and BMI of the patients were 56 years (±15) and 27.8 kg/cm2 (±5.3), respectively. All surgeries were successfully completed as planned without conversions to open surgery. No intra-operative complications or device deficiencies were observed, and one Clavien-Dindo IIIa postoperative complication occurred. The mean skin-to-skin operative time was 97 min (±46), the console time 73 min (±39) and docking time 2.2 min (±1.3).
Conclusion
Our experience with VHR utilizing DEXTER confirms its feasibility and safety, with operative times aligning with those reported in the literature for other robotic platforms. The Dexter system emerges as a valuable device in the toolkit of ventral hernia repair.
Robotic versus open mesh-enforced ventral hernia repair: a multi-center comparative study
Abstract
Background
Open mesh enforced ventral hernia repair is associated with increased surgical site occurrences (SSO) and prolonged hospital stay. A robotic-assisted minimally-invasive approach may offer benefits compared to open surgery, but comparative literature is scarce.
Aims
To report postoperative outcomes comparing open versus robotic mesh-enforced ventral hernia repair
Methods
This multi-center prospective cohort study used data from the international CROSSIFRE (MultiCentre InteRnational PrOSpective DatabaSe For Ventral HernIa REpair) register. All patients who underwent open or robotic mesh-enforced ventral hernia repair between December 2023 – November 2025 were analyzed using a 1:1 propensity score matching to adjust for body mass index (BMI), hernia size and type and component separation
Results
Ninety-three patients (34% female, median BMI 28.7kg/m2, 72% incisional hernias, median hernia diameter 4cm) underwent open repair and 93 patients (30% female, median BMI 28.4kg/m2, 68% incisional hernias, median hernia diameter 3.5cm; p=n/s) underwent robotic-assisted repair. Posterior component separation was performed in 31% open repairs and 26% robotic-assisted repairs (p=0.5). Median operation time was shorter in open repair compared to robotic-assisted repair (81min vs. 158min (p<0.001). Median length of hospital stay (LOS) was longer in open repair compared to robotic-assisted repair (3.5 days vs. 2days; p=0.006) and 30-day readmission rate was higher in open repair (9.7% vs. 0%; p=0.003). The rate of postoperative interventions and reoperations was higher in open repair compared to robotic repair (13% versus 1.1%; p=0.002 and 13% versus 0%; p<0.001, respectively).
Conclusion
This prospective comparative study indicates that robotic-assisted mesh-enforced ventral hernia repair offers clinically relevant perioperative benefits compared to an open approach with a shorter LOS, a lower readmission rate and fewer reinterventions and reoperations. Randomized controlled trials should be initiated to confirm these findings.
Comparative Outcomes of Laparoscopic and Robotic-Assisted Inguinal Hernia Repair: A Systematic Review of Randomized Controlled Trials
Abstract
Background
While conventional laparoscopic techniques, including totally extraperitoneal (TEP) and transabdominal preperitoneal (TAPP) repair, are well established, robotic-assisted approaches (rTEP/rTAPP) are increasingly adopted. However, the clinical and economic superiority in robotic inguinal hernia repair (IHR) remains unclear.
Aims
This systematic review compares outcomes of conventional laparoscopic versus robotic-assisted IHR.
Methods
A comprehensive literature search was conducted in Embase, MEDLINE, and the Cochrane Library to identify randomized controlled trials comparing robotic and conventional laparoscopic IHR. Four eligible trials (ROGER, RIVAL, ROLAIS, and VOLTAIRE), comprising 482 patients, were analyzed. Outcomes included operative time, surgeon workload assessed by the NASA Task Load Index (NASA-TLX), and postoperative complications.
Results
Baseline characteristics were comparable across studies regarding age, body mass index, and sex distribution. Surgeon proficiency requirements varied substantially between trials, ranging from twenty to over one hundred required previously performed procedures. Although all trials reported significant differences in operative time between approaches, only one demonstrated shorter duration with robotic surgery, resulting in a non-significant pooled estimate (MD 17.63; 95% CI −1.82 to 37.08). In total, robotic approach was associated with lower surgeon workload, although this result was not significant due to heterogeneous evidence in the individual studies (Figure 1; MD –4.50; 95% CI –16.78 to 7.78). Only one study reported significant differences in postoperative adverse events, favoring the robotic-assisted method. In summary, the complication rate did not differ significantly between laparoscopic and robotic-assisted approaches (OR 0.89, 95% CI 0.42 to 1.90).
Conclusion
Robotic-assisted IHR can offer workload benefits for surgeons compared to laparoscopic IHR without significantly increasing operative time and with comparable results regarding adverse events.
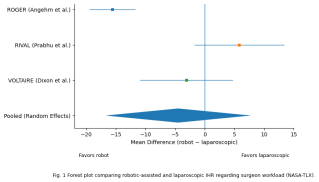
Safety and Patient-Reported Outcomes After suprapubic eTEP Robot-assisted Repair of Rectus Diastasis: A Single-Center Cohort Study
Abstract
Background
Postpartum rectus diastasis is common and may cause pain, core instability, functional impairment, and poor body image. Indications for surgical repair remain controversial. Minimally invasive and robotic techniques, including robotic-assisted eTEP suprapubic approach, expand options, but high-quality data on safety and patient-reported outcomes (PROMs) are limited. This study aimed to evaluate postoperative outcomes, safety, and patient-reported quality of life after robotic-assisted repair.
Aims
Assess safety, operative outcomes, complications, and patient-reported outcomes after robotic-assisted eTEP suprapubic repair.
Methods
All consecutive patients undergoing robotic-assisted repair of postpartum rectus diastasis with an eTEP suprapubic approach and retromuscular or preperitoneal mesh placement at a single center between 2018 and 2025 were retrospectively analyzed. Postoperative clinical outcomes and follow-up data were systematically reviewed. All patients completed validated PROMs, including the EuraHS-QoL, SF-36, and a Body Image Questionnaire. Primary endpoint was postoperative safety; secondary outcomes included operative time, complications, length of stay, and PROMs at follow-up
Results
Thirty-seven female patients were included; median age 42 years (IQR 38–47), ASA 2 (62%), median BMI 23.4 kg/m² (IQR 21.9–25.8). Median pregnancies: 2; pain was the main indication (78%). Concomitant hernias were present in 30 (81%) and repaired concurrently. Median operative time 189 min (IQR 165–215), hospital stay 3 days (IQR 2–4). Preoperative diastasis 55 mm (IQR 45–70), reduced to ≤5 mm (IQR 0–10) postoperatively. Mesh was used in all cases (median 20 × 10 cm, IQR 18 × 10–25 × 12 cm). Five patients (13.5%) had complications; one major (Clavien–Dindo IIIb) required reintervention. Median follow-up 18 months (IQR 12–30), 89% follow-up rate; no recurrences. PROMs showed low pain, minimal functional limitation, good physical function, and high body image satisfaction.
Conclusion
Robotic eTEP suprapubic repair of postpartum rectus diastasis with retromuscular/preperitoneal mesh and hernia repair appears safe, with low morbidity and favorable patient-reported outcomes
Combined Robotic-Assisted Ventral Hernia and Rectus Diastasis Repair: A Comparative Analysis of Primary versus Incisional HerniasCombined Robotic-Assisted Ventral Hernia and Rectus Diastasis Repair: A Comparative Analysis of Primary versus Incisional Hernias
Abstract
Background
Rectus diastasis frequently accompanies ventral hernias but is often undertreated. Combined robotic-assisted repair has emerged as a promising approach, yet comparative data on outcomes between primary and incisional hernias remain limited.
Aims
We evaluated the safety and efficacy of combined robotic-assisted ventral hernia and rectus diastasis repair in primary versus incisional hernias.
Methods
This retrospective analysis included 40 consecutive patients undergoing combined robotic-assisted ventral hernia and rectus diastasis repair (January 2018-July 2025), comprising 19 primary hernias (47.5%) and 21 incisional hernias (52.5%). All repairs utilized retromuscular mesh placement. Primary endpoint was perioperative safety by Clavien-Dindo classification. Secondary endpoints included technical success, operative time, hospital stay, and recurrence. Statistical analysis employed Mann-Whitney U test, Fisher exact test, and chi-square test (p<0.05).
Results
Baseline characteristics were comparable for age (p=0.13), sex (p=1.00), and body mass index (p=0.92). Incisional hernias had higher American Society of Anesthesiologists classification (28.6% vs 5.3% grade III, p=0.045) and larger defects (16.0 vs 4.8 cm², p<0.001). Technical success was 100% without conversions. Operative time was longer for incisional hernias (90 vs 72 minutes, p=0.016), yet hospital stay remained comparable (2 days, p=0.56). Overall complications occurred in 7.5% (3/40), exclusively in incisional hernias (14.3% vs 0%, p=0.23), all grade I seromas resolving spontaneously. No major complications, reoperations, or mortality occurred. At median follow-up of 478 days, no recurrences were observed (0%, p=0.34).
Conclusion
Combined robotic-assisted ventral hernia and rectus diastasis repair demonstrates excellent safety and efficacy for both primary and incisional hernias. Despite higher complexity in incisional hernias (higher risk classification, larger defects, longer operative time), outcomes remain comparable with low morbidity and no recurrences, supporting robotic-assisted repair across the spectrum of ventral hernia complexity.
Linea Arcuata Hernia: A Series of Three Cases of a Rare Internal Hernia
Abstract
Background
Linea arcuata hernia is an exceedingly rare type of abdominal wall hernia. Due to its deep anatomical location and nonspecific clinical presentation, linea arcuata hernias are frequently underdiagnosed or incidentally detected on computed tomography (CT).
Aims
The aim of this case series is to increase awareness of this rare entity and to correlate it with an accurate CT-based classification. This case series demonstrates the heterogeneity of linea arcuata hernias and emphasizes their inclusion in the differential diagnosis of lower abdominal pain.
Methods
On CT imaging, three morphological forms can be distinguished:
-
Isolated preperitoneal fat protrusion beneath the arcuate line
-
A true hernia sac containing omentum or bowel
-
A combined or advanced form characterized by a significant fascial defect with visceral involvement
We present three cases of linea arcuata hernia.
The first case involved a class 3 hernia with an additional ipsilateral trocar-site hernia and was treated using using a robotic transabdominal approach with partial transversus abdominis release.
The second case consisted of a class 2 hernia associated with bilateral femoral hernias, a contralateral Spighelian hernia, and an umbilical hernia, and was managed via a totally extraperitoneal laparoscopic approach.
The third case was an intraoperative finding of a class 1 linea arcuata hernia during laparoscopic preperitoneal umbilical hernia repair, requiring wider dissection and extended mesh coverage.
Results
Two of the patients were symptomatic and reported recurrent lower abdominal pain on the affected side. Only CT scan revealed the diagnosis of linea arcuata hernias. The cases presented demonstrate variability in radiological appearance as well as differences in surgical strategies.
Conclusion
These cases highlight the heterogeneity of linea arcuata hernias in both radiological appearance and surgical management. Awareness of this rare condition and precise CT-based classification are crucial for accurate diagnosis and optimal surgical planning.


Occult Femoral Hernias Are Frequently Underdiagnosed:
Findings across Laparoscopic, Robotic, and Open Approaches
Abstract
Background
Femoral hernias represent an important subgroup of groin hernias frequently underdiagnosed preoperatively. According to the European Hernia Society Guidelines, clinical examination has limited sensitivity for femoral defects, and even cross-sectional imaging may fail to detect them. Laparoendoscopic approaches provide superior visualization of the myopectineal orifice, enabling identification of femoral hernias. To date, comparative data on the detection of occult femoral hernias across different surgical techniques remain limited.
Aims
This study aims to evaluate the incidence of occult femoral hernias and to assess differences in detection between open, laparoscopic and robotic approaches.
Methods
Retrospective analysis of patients undergoing groin hernia repair (inguinal and femoral) at a tertiary university surgical department between 2018–2024. Surgical approaches included laparoscopic repair (TAPP/TEP), robotic-assisted repair, and open repair (e.g. Lichtenstein/Stoppa). Occult femoral hernia was defined as a femoral defect identified intraoperatively without preoperative documentation on clinical assessment or imaging. Parameters included hernia characteristics, preoperative imaging findings, intraoperative findings, and postoperative outcomes.
Results
Among 148 patients (27 women, 121 men), occult femoral hernias occurred 29 times and, thereby, constituted 19.6% of groin hernia repairs. Detection of occult femoral hernia occurred predominantly during laparoscopic repair (22/29), followed by open repair (6/29) and robotic-assisted repair (1/29). No occult femoral hernia was documented preoperatively despite frequent imaging. Postoperative pain was reported in 31.0% of patients with occult femoral hernia at a mean follow-up of 172 days. Complications were rare; one seroma required reoperation.
Conclusion
Occult femoral hernias remain underdiagnosed despite routine clinical and radiological assessment. Both laparoscopic and robotic-assisted approaches allowed intraoperative identification of occult femoral hernias, reinforcing their role as possible preferred modalities for groin hernia repair. Increased awareness of the prevalence and morphology of occult femoral hernias may improve surgical planning, informed consent of patients, and surgical outcomes.
Gender-Based Differences and the Impact of Surgical Techniques on Postoperative Outcomes in Groin Hernia Surgery
Abstract
Background
Women are less frequently affected by inguinal hernias than men and are underrepresented in clinical studies, despite evidence suggesting a higher risk of postoperative complications such as chronic pain and recurrence. This highlights the need for a gender-sensitive evaluation of surgical techniques and postoperative outcomes in groin hernia surgery.
Aims
The aim of this ongoing study is to investigate gender-specific differences in surgical management, and outcomes, with particular emphasis on female patients.
Methods
This retrospective single center study included all consecutive patients undergoing surgical repair of inguinal and/or femoral hernias at a tertiary university surgical department between 2018-2024. Demographics, surgical techniques and postoperative outcomes. Demographics, surgical techniques, and postoperative outcomes, including complications, recurrence, and postoperative pain, were analyzed.
Results
A total of 148 patients were included, of whom 18.2% were women. No significant differences were observed between women and men with respect to age (mean 59 vs. 57.7 years) or body mass index (26 vs. 25.5 kg/m²). Mean operative time was longer in women compared with men (105.7 vs. 97 minutes), although this difference did not reach statistical significance. Postoperative pain occurred significantly more frequently in women than in men (p = 0.031). Spontaneous resolution of postoperative pain was observed in 5 of 19 women and 4 of 20 men, with a mean time to resolution of 287 days in women and 307 days in men. No significant sex-based differences were found regarding preoperative pain or subjectively disturbing swelling (p = 0.173). Total extraperitoneal endoscopic repair was the most frequently performed technique in both groups, followed by Lichtenstein, Stoppa, and transabdominal preperitoneal (TAPP) repair.
Conclusion
Women remain underrepresented among patients undergoing inguinal and femoral hernia repair; however, postoperative pain occurs significantly more frequently than in men. Postoperative pain in women may be more frequently self-limiting and resolve earlier. A prospective multicenter study is planned to further elucidate gender-specific differences in postoperative pain trajectories following groin hernia surgery.
Joining Forces for Education and Training – Building the Next Generation of Thoracic Surgeons
The Trainees’ Perspective
The Trainers’ Perspective
Approaches to a National Strategy to Improve Training in Thoracic Surgery
Lessons From the Wild Wild West: the CURCT Approach
The future of training in thoracic surgery in Switzerland
One World, One Scalpel: Rethinking Surgery Beyond Borders
Beyond the Knife: Perioperative Care as the True Cornerstone of Surgery
Global Surgery Beyond Declarations: Who Really Delivers Essential Surgical Care?
Training Where It Matters: Reflections on Local Capacity Building in Malawi
Feasibility of Laparoscopic Surgery in a Low-Resource Pacific Island Hospital: Early Experience
OR TEAM: Joining Forces Every Day!
This session is in French, but the session will be translated by an AI translation app. Bring your smartphone and headphones to experience the translation.
Collaboration interprofessionnelle lors de la mise en œuvre de la PIPAC en chirurgie colorectale
Projet Teamstepps: SBAR au bloc opératoire
Serious Games : Mission stop infection : le défis du bloc!
Antisepsie post-incisionnelle de la littérature à la pratique
STS – Free Communication 1
Preventing Cerclage Failure: How Many Twists Are Needed to Avoid Untwisting and Maximize Fixation Strength
Abstract
Background
Cerclage wires are widely used for fixation of long-bone spiral and peri-implant fractures. However, the optimal number of twists to maximize biomechanical stability is not defined and is largely based on surgical experience. This study investigated the influence of twist number and wire diameter on cerclage stability.
Aims
To determine how twist number and wire diameter affect failure mode, stiffness, and load-bearing capacity of cerclage wires, and to identify the minimum twist number required to prevent untwisting.
Methods
A total of 120 stainless-steel cerclage constructs were produced using 1.0-mm, 1.25-mm, and 1.5-mm wires with 4, 6, 8, or 10 twists. Twist formation was standardized with controlled axial load of torque, followed by uniform trimming. Static tensile testing assessed stiffness, load-to-yield, elongation, and load-to-failure. Hand-twisted 1.5-mm constructs underwent cyclic loading at 700 N until elongation of 2, 3, or 5 mm or catastrophic failure.
Results
Across all diameters, low twist counts failed predominantly by untwisting, while higher twist counts shifted failure toward wire breakage. In 1.0-mm wires, breakage occurred only at 10twists (50%), whereas all lower twist counts failed by untwisting (p=0.040). In 1.25-mm wires, breakage appeared only at 8 and 10twists (p>0.9). Stiffness increased with twist number: 1.0-mm wires from 34.1±2.4 N/mm (4twists) to 41.5±5.0 N/mm (10 twists); 1.25-mm from 44.0±5.5 to 50.5±5.4 N/mm; and 1.5-mm peaked at 8 twists (92.8±17.0 N/mm) before decreasing at 10 twists (82.3±11.8 N/mm). Load-to-failure increased with diameter and twist number, reaching 660.7±139.6 N (1.0-mm, 10 twists), 858.0±220.0 N (1.25-mm, 8twists), and 1873.7±80.6 N (1.5mm, 10twists). In cyclic testing, six-twist 1.5-mm constructs showed the greatest durability, requiring the most cycles to reach 2,3,and 5mm elongation.
Conclusion
Increasing twist number consistently shifts failure from untwisting to wire breakage. Six to eight twists provide optimal biomechanical performance, with six twists representing the minimum required to prevent untwisting across all clinically used wire diameters.
The Prefabricated MFC–SCIP Chimeric Flap: An Engineered Approach to Reconstruction
Abstract
Background
Complex composite defects of the upper limb resulting from trauma, infection, multiple surgeries, or tumors remain a major reconstructive challenge. While staged reconstruction is often considered standard, it exposes patients to repeated procedures, prolonged hospitalization, and delayed rehabilitation. Advances in microsurgery have enabled multi-tissue and chimeric flaps; however, these may be limited by local tissue availability or insufficient volume in extensive defects. Fabricated chimeric flaps—constructed by microsurgical assembly of tissues from different donor sites—represent an emerging concept at the frontier of microsurgical reconstruction, though clinical experience remains scarce.
Aims
This study presents a series of five patients undergoing complex upper limb reconstruction using a fabricated chimeric flap combining a medial femoral condyle (MFC) corticoperiosteal flap with a superficial circumflex iliac artery perforator (SCIP) flap. The aim was to evaluate feasibility, reliability, and clinical outcomes.
Methods
Between 2021 and 2024, five consecutive patients with composite upper limb defects underwent single-stage reconstruction. Defects involved the wrist (n=3), elbow (n=1), and clavicle (n=1). A corticoperiosteal MFC flap based on the descending genicular artery was combined with a SCIP skin paddle through microsurgical prefabrication. Outcomes included flap survival, radiological bone consolidation, complications, and functional results. Follow-up was performed using serial radiographs and computed tomography.
Results
Mean follow-up was 31 months. Complete survival of the soft-tissue component was achieved in all cases. Bone integration was obtained in four patients; one case of nonunion required salvage wrist shortening and fusion. No total flap loss occurred. Functional assessments and patient-reported outcomes were favorable in all patients achieving bone consolidation.
Conclusion
The prefabricated chimeric MFC–SCIP flap allows reliable single-stage reconstruction of complex upper limb osteocutaneous defects, offering high osteogenic potential, robust soft-tissue coverage, and satisfactory functional outcomes.
Long term outcome after spanning plate for distal radius fractures
Abstract
Background
Minimal invasive temporary spanning plate fixation has been established as a valuable treatment method for complex distal radius fractures. While short-term outcomes are promising, data on long-term results remain limited.
Aims
The purpose of this study is to conduct a long-term outcome analysis of patients treated with SP fixation, representing the longest follow-up period documented in current literature.
Methods
We retrospectively analyzed spanning plate fixation for complex distal radius fractures at a level I trauma centre (2018–2024). Patients with minimum one-year follow-up were assessed using PRWE, VAS, and satisfaction scores, while monitoring complications like CRPS and tendon ruptures (Figure 1).
Results
A total of 35 patients (Table 1) met the inclusion criteria, with 26 patients available for long-term follow-up (Table 2). The average age was 57 years (range 22–92) and 89% of fractures were classified as AO type C. The SP was removed on average 3.8 months postoperatively. The mean follow-up period was 58.3 months (range 13–90 months). Radiological fracture union was achieved in all patients with a mean time to union of 8.5 weeks. Complications included one implant failure due to renewed trauma and one Extensor Pollicis Longus (EPL) rupture in a patient where the tendon was not superficialized. There were no cases of surgical site infection. The mean satisfaction score was 4.1 (range 2–5) and the mean Visual Analog Scale (VAS) for resting pain was 1.7. The mean PRWE score was 16.7 (Table 3).
Conclusion
The radiological, functional, and patient-rated outcomes in this study confirm that the excellent results observed in the short term are successfully maintained over a long-term period of 4.5 years. The spanning plate technique proves to be a reliable and durable treatment option for complex distal radius fractures with a low long-term complication rate.
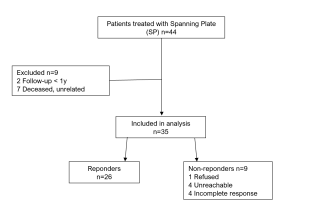
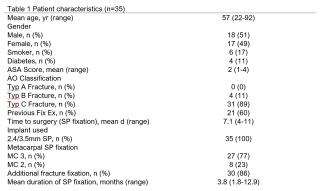
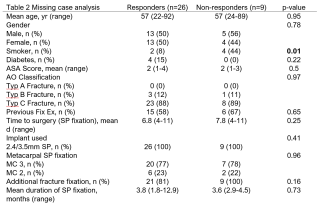
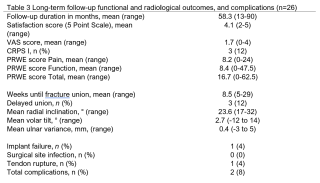
MIPO Versus ORIF for Proximal Humerus Fractures: Comparison of Functional Outcomes Between Two Conceptually Distinct Operative Approaches
Abstract
Background
Minimally invasive plate osteosynthesis (MIPO) and open reduction and internal fixation (ORIF) are widely used approaches for proximal humerus fractures, reflecting distinct philosophies of soft-tissue preservation and direct anatomic control. Despite decades of refinement, it remains unclear whether these differences translate into meaningful differences in recovery. Interpretation of existing comparisons is limited due to technique selection commonly reflecting fracture complexity, surgeon preference, and experience, resulting in substantial confounding by indication.
Aims
To compare functional outcomes after MIPO and ORIF for proximal humerus fractures at six weeks and one year within a natural-experiment framework.
Methods
The study included operatively treated patients with displaced proximal humerus fractures from a cohort characterised by expert disagreement on operative versus nonoperative management. Treatment allocation was determined by geographical catchment area: patients treated at one centre routinely underwent MIPO, whereas those treated at another underwent ORIF, assigning technique independently of surgeon choice or fracture characteristics. Functional outcomes were assessed at six weeks and one year using validated patient-reported measures (QuickDASH, EQ-5D index and health score, Subjective Shoulder Value, and pain NRS). Multivariable analyses adjusted for age, ASA classification, and Neer fracture type; complications and reoperations were recorded.
Results
Eighty-four patients were included (MIPO 57, ORIF 27), with high follow-up completeness. No clinically relevant differences were observed in functional outcomes at six weeks or one year. Both groups improved substantially with parallel recovery trajectories. Revision rates were low and comparable (10.5% vs 11.1%). Implant removal was more frequent after MIPO (31.6% vs 7.4%), largely reflecting elective, protocol-driven practice rather than complication-related reoperations.
Conclusion
When evaluated as mature, centre-embedded treatment pathways rather than isolated techniques, MIPO and ORIF yield equivalent functional recovery and comparable safety profiles. Operative choice should therefore be guided less by theoretical advantages of exposure or soft-tissue preservation and more by surgeon expertise, organisational consistency, and downstream planning, including conversion to arthroplasty.
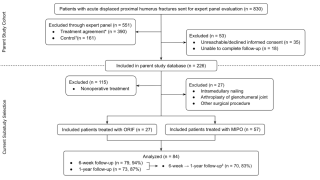

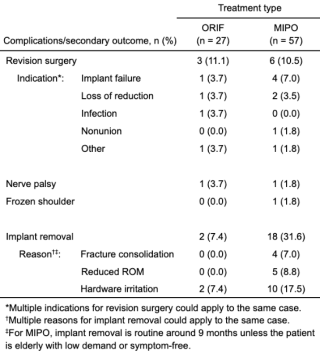
Influence of Cemented Femoral Stem Design on the Risk of Periprosthetic Femoral Fractures: A comparative retrospective study
Abstract
Background
Periprosthetic femoral fractures (PPFx) are an increasingly common complication after hip arthroplasty and a major cause of revision surgery. Although cemented femoral stems are generally associated with a lower fracture risk than uncemented designs, the influence of cemented stem geometry and cementation technique on long-term fracture incidence remains insufficiently defined. The classification proposed by Hegde et al. (2024) differentiates cemented stems into polished taper-slip (Type I) and composite-beam (Type II) designs, but comparative clinical data remain limited.
Aims
The primary aim of this study was to compare the risk of periprosthetic femoral fracture between Type I cemented stems implanted using traditional cementing versus line-to-line cementing techniques. Secondary objectives were to compare fracture risk between cemented and uncemented stems and to identify additional risk factors, including stem material and geometry.
Methods
This retrospective registry study analysed nationwide data from 2015 to 2024 obtained from the Swiss Implant Registry (SIRIS), which captures all hip arthroplasties performed in Switzerland. Cemented stems were classified according to the Hegde system. Multivariable regression models were used to assess associations between stem design, cementation technique, implant material, patient-related variables, and the risk of periprosthetic femoral fracture at different postoperative time points.
Results
A total of 223,959 primary hip arthroplasties were included. Fracture incidence differed significantly between stem categories, with Type I cemented stems showing a higher risk of periprosthetic femoral fracture than Type II stems. Within the Type I group, line-to-line cementing was associated with a higher fracture risk compared with traditional cementing. Regarding stem geometry, straight stems demonstrated the lowest fracture incidence, while gradual taper designs, followed by quadruple-taper stems showed the highest risk.
Conclusion
Femoral stem design and cementation technique significantly influence the PPFx risk. Large-scale registry analysis highlights relevant design-related differences that may inform stem selection and reduce fracture incidence. Prospective studies are warranted.
Assessing Surgical Skill in Orthopedic Trauma Surgery Training: Behavioral Metrics for Digital Performance Evaluation
Abstract
Background
Surgical skill assessment in orthopedic trauma surgery still relies on subjective expert ratings, limiting consistency and scalability. Although digitalization offers opportunities for objective evaluation, the manual and haptic nature of surgery makes digital capture of tool use challenging, keeping such approaches underdeveloped.
Aims
This study introduces a digital framework that uses optical tracking to create a digital twin of surgical real-world procedures with realistic haptics, enabling extraction of digital behavioral metrics (DBM). It investigates (1) which DBM reflect technical proficiency and (2) how well these metrics predict surgical performance compared to expert assessment.
Methods
28 participants performed three standardized fracture fixations on synthetic bone models of the radius, ulna, and fibula. Tool motion was captured and transformed into a digital twin from which metrics such as path length, smoothness, and task duration were derived. (Figure 1) These metrics were statistically compared to benchmark performance scores, defined as the average of four expert ratings using the Global Rating Scale (GRS). (1) Correlation analysis identified skill-relevant metrics, and (2) a predictive model was trained to estimate performance from DBM evaluating its accuracy against the expert ratings.
Results
(1) Several DBM were found to be indicative of surgical performance. Measures based on tool path length and time per activity showed strong correlations with expert ratings, reaching coefficients of up to 0.6. Correlation strength varied across tools and procedures. (Figure 2) (2) The predictive model achieved a mean absolute difference from the benchmark score of 3.8 on the GRS scale (range: 28–70 points), outperforming the average inter-expert difference of 4.6 points. (Figure 3)
Conclusion
DBM were identified as valid indicators of surgical skill. Their predictive performance exceeded the agreement between individual experts, demonstrating the potential for objective, expert-independent assessment using digital performance evaluation frameworks.
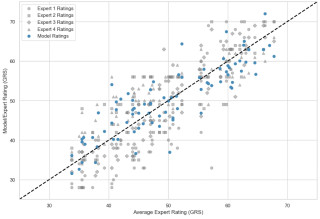


Is There a Relation Between Muscle Mass Surrounding Fractures and Acute Compartment Syndrome Incidence? A Retrospective Cohort Study Examining Extra-Articular Tibial Fractures.
Abstract
Background
Acute compartment syndrome (ACS) following tibial fractures is a frequent and potentially catastrophic complication when not promptly identified.
Aims
The aim of this study was to compare muscle mass and ACS incidence rate around extra-articular tibial fracture sites. This could potentially highlight muscle mass as an ACS risk factor.
Methods
This retrospective cohort study was performed in a level I trauma center and included 614 extraarticular tibial fractures occurring between 01/01/2005 and 12/31/2019 in 559 patients older than 16. Fractures classified as AO/OTA 41-A, 42-A, 42-B, 42-C and 43-A were eligible. The tibia was arbitrarily divided into 8 equally long bony segments, and each fracture was allocated to one of these segments depending on the localization of its center. For each tibial segment, an ACS incidence rate was determined. Alternatively, muscle mass surrounding the same 8 equally long tibial segments was measured on a series of 31 patients having undergone bilateral fine cut computed tomography scans of the legs. These measurements were obtained from healthy limbs (no past surgery, no ancient or recent trauma, no active or sequelar infection, no tumoral condition, no systemic disease with muscular involvement) using a semi-automatic tool in Osirix (ROI volume/compute volume) with manual drawing and automatic propagation of measurements of muscle volume.
Results
Figure 1 shows ACS incidence rates using a LOESS (locally estimated scatterplot smoothing) curve and mean muscle volumes associated to each of the 8 tibial segments.
Conclusion
When comparing ACS incidence rate and muscle volume curves, a similarity is visible as both curves increase initially and then slope down. Because both cohorts of patients were different and heterogenous, a purely mathematical or statistical comparison is not possible. However, descriptive comparison of both curves may lead to the conclusion that the more muscle mass is around a fracture site, the more chances there are of developing ACS.

Old Versus New Generation Plates in Distal Radius Fractures: Impact on Implant Removal Rates
Abstract
Background
Distal radius fractures are among the most common fractures in the human body, with incidence increasing worldwide. Advances in surgical techniques and implant design have led to widespread use of variable-angle volar locking plates, allowing stable fixation and anatomical reduction even in complex fracture patterns. Despite ongoing innovation, it remains unclear whether newer-generation implants provide meaningful clinical advantages or reduce the need for secondary implant removal after fracture healing.
Aims
The aim of this study was to compare old- and new-generation volar locking plates in the treatment of distal radius fractures, focusing on implant removal rates, postoperative complications, and plate positioning.
Methods
This retrospective study included patients treated between June 2019 and June 2022 at a level I trauma center in Switzerland. All distal radius fractures managed with variable-angle volar locking plates either from Synthes, Medartis or Arthrex were eligible. Synthes plates were classified as old-generation implants, whereas Medartis and Arthrex plates were considered new-generation designs. Patients were grouped according to implant generation. The primary outcome was implant removal for any indication, including volar irritation or patient request. Secondary outcomes included postoperative complications at one year.
Results
A total of 213 cases were analyzed, with 64 patients in the old-generation group and 149 in the new-generation group. The new-generation group included significantly more complex fractures (68.5%, p < 0.001) and greater surgeon experience (58.4% vs. 32.8%, p = 0.001). Implant removal rates did not differ between old-generation (24.2%) and new-generation plates (26.6%, p = 0.731). The distance between the distal plate edge and the volar lip of the radius was shorter in the new-generation group (2.4 ± 0.9 mm vs. 2.8 ± 0.9 mm, p = 0.027). Postoperative complication rates were comparable.
Conclusion
These findings indicate that newer-generation volar locking plates do not reduce implant removal rates or complications compared with older designs.
Supervised or Unsupervised Physiotherapy After Distal Radius Fracture Surgery: Is Supervision Worth the Cost?
Abstract
Background
This systematic review and meta-analysis evaluated the effectiveness of traditional face-to-face physiotherapy (supervised [SP]) compared with home exercise programs supported by paper handouts, instructional videos, or smartphone applications (unsupervised [UP]) in the postoperative rehabilitation of patients with surgically treated distal radius fractures.
Aims
The primary aim of this study is to determine whether unsupervised or supervised physiotherapy after operative treatment of distal radius fractures yields more favorable results in terms of Patient-Rated Wrist Evaluation (PRWE) scores, pain, and range of motion (ROM).
Methods
A comprehensive search of PubMed, Embase, and the Cochrane Library identified randomized controlled trials comparing supervised and unsupervised physiotherapy following osteosynthesis of distal radius fractures. The primary outcome was wrist function and pain assessed by the Patient-Rated Wrist Evaluation (PRWE). Secondary outcomes included the Disabilities of the Arm, Shoulder and Hand score (qDASH), range of motion (ROM), grip strength, and postoperative complications.
Results
Nine trials comprising 470 patients met the inclusion criteria. Across all time points, no significant differences were observed between the SP and UP groups, except for the PRWE score at 12 weeks, which slightly favoured the SP group (12.2 [95% CI: 9.8–14.7] vs. 16.0 [95% CI: 13.8–18.1]). However, this difference did not exceed the minimal clinically important difference (MCID) of 11.5 points. Aftercare-related complications occurred in 1.1% of patients in both groups, with complex regional pain syndrome (CRPS) being the most common (SP 3.4% vs. UP 4.9%). Subgroup analysis indicated a non-significant but clinically relevant trend toward worse PRWE scores at six weeks among patients aged over 60 years.
Conclusion
Supervised and unsupervised physiotherapy yielded comparable outcomes in wrist function, pain, and complications after distal radius fracture surgery. Although the SP group demonstrated a statistically significant advantage in PRWE at 12 weeks, this difference is unlikely to be clinically meaningful. Older patients, however, may experience inferior functional recovery with unsupervised programs.
When Disaster Strikes, the Time to Prepare Has Passed. Are You Ready?
Meet the Expert – All About Career, Training in a Swiss Hospital - with Tenzin Lamdark
When Disaster Strikes, the Time to Prepare Has Passed. Are You Ready?
Open Discussion: "Meet the Expert"
*Scientific Programme is Subject to change






